Radial Head Fractures
Dr. KS Dhillon
Introduction
Radial head fractures are common intra-articular fractures of the elbow. They can be associated with an injury to the distal radioulnar joint and/or to the interosseous membrane (Essex-Lopresti).
Diagnosis is made with x-rays of the elbow. CT scans can be useful for surgical planning.
Treatment is nonoperative for undisplaced fractures without a mechanical block to motion. For displaced fractures or fractures associated with mechanical block to motion or elbow/forearm instability, the treatment is surgical.
Etiology
The radial head fracture results from a fall on an outstretched hand with the
elbow in extension and forearm in pronation. During such a fall the most force is transmitted from the wrist to the radial head.
The incidence of associated injuries is about 30%. These include associated soft tissue injuries and skeletal injuries. The ligamentous and interosseous injuries include:
Lateral collateral ligament (LCL) injury is the most common with up to 80% on MRI
Medial collateral ligament (MCL) injury
Essex-Lopresti injury-- radial head fracture with distal radioulnar joint (DRUJ) injury and interosseous membrane injury
Elbow fractures & dislocations-- coronoid fracture, olecranon fracture, Monteggia fracture/dislocation, and the terrible triad of posterolateral elbow dislocation, radial head fracture, and coronoid fracture
Carpal fractures- scaphoid fracture
Anatomy
The proximal radius consists of:
radial head
radial neck
radial tuberosity
radial shaft
The radial head is 15º offset from the neck. The anterolateral third of the radial head lacks subchondral bone and is easily fractured in this area.
The articular surface has an oval-shaped concavity that articulates with the capitellum of the humerus. The nonarticular portion of the radial head is
considered a safe zone for hardware placement.
The radiocapitellar joint is a pivot joint. Sixty percent of the load transfer across the elbow joint passes through this joint. A fracture or resection of the radial head decreases the surface area available for load transfer and decreases the stability of the elbow.
The ulnar portion of the radial head articulates with the lesser sigmoid notch of the ulna to form the proximal radial ulnar joint (PRUJ). This joint is important for pronation and supination of the forearm.
The ligaments at the elbow (fig1) include the lateral collateral ligament complex and the medial (ulnar) collateral ligament (MCL). The lateral collateral ligament complex consists of the lateral ulna collateral ligament (LUCL), the radial collateral ligament (RCL), the annular ligament, and the accessory lateral collateral ligament.
The lateral ulnar collateral ligament arises from the lateral epicondyle and inserts onto the supinator crest of the ulna. It is the primary stabilizer to varus and external rotation (hypersupination) stress. It is a more important stabilizer near elbow extension. Its deficiency results in posterolateral rotatory instability.
The radial collateral ligament inserts into the annular ligament. The annular ligament originates on the anterior aspect of the lesser sigmoid notch and inserts on the posterior aspect of the lesser sigmoid notch. It stabilizes the proximal radioulnar joint by maintaining the radial head in contact with the ulna.
One-third of individuals have an accessory lateral collateral ligament (ALCL) which runs from the annular ligament to the supinator crest of the ulna.
The medial (ulnar) collateral ligament (MCL) consists of three bundles, the
anterior bundle, posterior bundle, and transverse bundle. It is the primary stabilizer to valgus stress (radial head is second). The anterior bundle arises from the inferior margin of the medial epicondyle and inserts at the sublime tubercle of the ulnar coronoid process. It is composed of a superficial and a deep layer. The transverse bundle originates from the proximal medial olecranon and runs distally to insert just distal to the coronoid. This ligament originates and inserts on the ulna, hence it does not provide significant stability. The posterior bundle originates at the posterior aspect of the medial epicondyle of the humerus and attaches to the medial aspect of the olecranon process, and it forms the floor of the cubital tunnel.

Fig 1- Ligaments of the elbow
Biomechanics
The radial head confers two types of stability to the elbow, valgus stability and longitudinal stability. The radial head is a secondary restraint to the valgus load at the elbow. It is important if MCL is deficient.
The longitudinal stability is a restraint to the proximal migration of the radius. There are contributions from the interosseous membrane and DRUJ.
The load-sharing from the wrist to the radiocapitellar joint is dependent on the radiocapitellar surface area. A loss of longitudinal stability occurs with the Essex-Lopresti injury pattern where there is a radial head fracture, DRUJ injury, and interosseous membrane disruption. The radial head must be fixed or replaced to restore stability and prevent proximal migration of the radius and ulnocarpal impaction.
Classification
The commonly used classification is the Mason Classification which was
modified by Hotchkiss and Broberg-Morrey:
Type I- Nondisplaced or minimally displaced (<2mm) fracture with no mechanical block to rotation
Type II- Displaced >2mm or angulated fracture with possible mechanical block to forearm rotation
Type III- Comminuted and displaced fracture with a mechanical block to motion
Type IV- Radial head fracture with associated elbow dislocation
The advanced classification is the OTA Classification
2R1A- Extra-articular pattern
2R1B- Partial articular pattern
2R1C- Complete articular pattern
Clinical Presentation
The most common symptom is pain. Examination shows tenderness along the lateral aspect of the elbow with limitation of elbow and forearm motion, particularly supination/pronation.
Inspection of the limb will show ecchymosis and swelling over the lateral aspect of the elbow. A deformity will be seen if there is elbow dislocation. A mechanical block to elbow motion must be looked for. Aspiration of joint hematoma and injection of local anesthesia helps in the evaluation of mechanical block.
Stability testing of the elbow is carried out. The posterolateral drawer test, posterolateral pivot shift test (tests LUCL), and valgus stress test (tests MCL) are carried out.
For DRUJ injury, palpate the wrist for tenderness. Any translation in the sagittal plane of more than 50% compared to the contralateral side is abnormal. If difficult to determine DRUJ injury on examination, a dynamic CT scan in neutral, pronation and supination can be done.
For interosseous membrane injury palpate along the interosseous membrane for tenderness.
Imaging
The recommended x-rays include AP and lateral view of the elbow and
AP and lateral views of the forearm/wrist.
A fracture with or without displacement and with or without intra-articular involvement can be seen. Anterior and or a posterior fat pad sign can be seen in patients with occult minimally displaced fracture of the radial head.
The fat pad sign indicates the presence of intra-articular hemarthrosis. The posterior fat pad sign is more sensitive for a fracture.
A radiocapitellar view or Greenspan view (fig 2) can be useful for the diagnosis of a radial head fracture. It is an oblique lateral view of the elbow that is taken with the beam angled 45 degrees cephalad. It allows visualization of the radial head without coronoid overlap. It helps detect subtle fractures of the radial head.
A CT scan is carried out for comminuted fractures to further delineate the fracture fragments. It is also useful in patients with complex fracture dislocations. The CT scan can be helpful in planning surgical techniques and approaches.
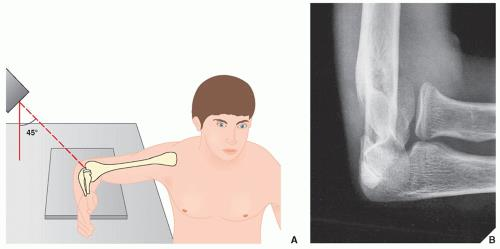
Fig 2- Radiocapitellar view or Greenspan view
Treatment
Nonoperative Treatment
Isolated minimally displaced fractures with no mechanical block (Mason Type I) are treated with short periods of immobilization for 3-7 days. Early mobilization is necessary to prevent elbow stiffness. The outcome is generally good with good results in 85% to 95% of patients.
Operative Treatment
Open reduction and internal fixation (ORIF) is indicated in:
Mason Type II fracture with mechanical block
Mason Type III fracture where ORIF is feasible
When there are other complex ipsilateral elbow injuries
The fractures can be fixed with screws alone or with a plate and screws depending on the type of fracture.
The outcome is generally good to excellent in more than 90% of the patients with Mason II fractures. The outcome of Mason III fractures is variable.
The outcome of open reduction and internal fixation is worse when there are more than 3 fragments as compared to when there are less than 3 fragments. Unsatisfactory outcome is seen in more than 50% of patients following ORIF in patients with more than 3 fragments.
There is no significant difference in outcome at 4 years in patients who had
ORIF of isolated radial head fractures versus complex radial head fractures. Isolated fractures, however, have a better Patient-Rated Elbow Evaluation score, lower complication rate, and lower rate of secondary capsular release.
Partial excision of the radial head or fragment excision can be carried out in
older, lower demand patients with complex fractures who have no associated instability. Fragments less than 25% of the surface area of the radial head or 25%-33% of capitellar surface area can be excised.
Sometimes even small fragment excision can lead to instability.
Complete excision of the radial head is carried out in low demand, sedentary patients. In a delayed setting complete excision of the radial head is carried out for continued pain due to an isolated radial head fracture.
Complete excision of the radial head is contraindicated in patients with
destabilizing injuries such as forearm interosseous ligament injury (>3mm translation with radius pull test), coronoid fracture, and medial collateral deficiency.
The outcome after radial head excision is worse with regard to strength, function, and motion when compared to open reduction and internal fixation. The incidence of osteoarthritis after excision of the radial head is as high as 73% when compared to the contralateral uninjured elbow.
Radial head arthroplasty is indicated in patients with:
Comminuted fractures (Mason Type III) with more than 3 fragments
Severe plastic deformity of the radial head
Nonunion/malunion
Elbow fracture-dislocations with terrible triad or Monteggia variants and with involvement of more than 30% of the articular surface of the radial head
Essex-Lopresti lesions- radial head excision will exacerbate elbow/wrist instability and may result in proximal radial migration and ulnocarpal impingement
Radial head fractures that require replacement have shown good clinical outcomes with metallic implants. Compared to ORIF for fracture dislocations and Mason Type III fractures, arthroplasty provides greater stability, lower complication rate, and higher patient satisfaction.
Indications and outcomes of radial head excision
The most common indication for primary excision of the radial head is acute comminuted fracture of the radial head. In the chronic setting rheumatoid arthritis is a common indication.
The literature comparing radial head excision to ORIF in the acute setting is less conclusive. There are two studies in the literature. One study found no significant differences, and one found significant differences favoring ORIF only in certain outcome measures such as grip strength and forearm rotation. Hence, there is not enough data to support one procedure over the other, even though from a clinical point of view ORIF is typically performed for those fractures involving less than three fragments that are amenable to fixation [1]. In the chronic setting also the conclusions are unclear.
The results of secondary excision of the radial head following trauma showed a relatively high rate of post-operative pain, low satisfaction, and a high rate of giving up sports and jobs. This, however, was supported only by two studies. One study comparing primary excision within three weeks to secondary excision found that the best results were obtained after primary excision [2].
Most of the published studies conclude that radial head excision results in favorable long-term outcomes when used to treat isolated displaced and comminuted radial head fractures. It is important to evaluate the elbow for associated injuries prior to resection of the radial head, particularly ligamentous injuries because the outcomes in this group has been reported to be poor [3-7]. Radial head excision is contraindicated in patients with MCL or interosseous membrane injuries unless these injuries are concurrently treated.
Several studies have shown that the long-term (more than 14 years) outcome of radial head excision was good and that it was a viable treatment option with good functional results [3,6,8,9,10,11].
Radial head excision does have some long-term complications. These include osteoarthritis of the elbow, valgus instability, stiffness, and proximal migration of the radius.
Advanced osteoarthritic changes are often present following radial head excision but typically these radiographic findings are not associated with functional impairment [9,12]. The degenerative grading does not necessarily correlate with clinical outcome [13].
Some long-term follow-up studies demonstrate valgus instability, stiffness, or proximal migration of the radius following radial head excision [14,15]. Excision of the radial head leads to a very low complication rate, with low-clinical-impact radiographic arthritis being the most significant one. There is not much literature comparing the outcome of radial head excision to radial head replacement for acute treatment of the radial head fracture. There is only one study that compared radial head excision to replacement. The study found no difference between the two treatments in terms of functional scoring but did find that extension was significantly more restricted in the replacement group [16].
There are several studies in the literature that assessed outcomes of radial head replacement for fracture with a mean follow-up of eight years or more. All the studies reported sustained good or excellent clinical results with few complications [17-20]. The contention of whether radial head replacement or excision is a better treatment for acute trauma cases remains a grey area, except where excision is contraindicated such as in situations when valgus or axial instability is present [21].
In conclusion, the primary indication for radial head excision is fracture comminution in the acute setting. The outcome is generally good or excellent following radial head excision for radial head fractures. There is insufficient evidence to recommend ORIF or replacement compared to radial head excision in patients with complex radial head fractures. Radial head excision should not be performed when there are concurrent ligamentous injuries of the elbow. Secondary radial head excision in posttraumatic situations produces inferior results and patients often continued to have residual pain.
Treatment Techniques
1. Nonoperative management
An arm sling or posterior long arm splint can be used for 3-7 days followed by early mobilization of the elbow to prevent stiffness.
2. Open reduction and internal fixation (ORIF)
Approaches
There are several approaches for open reduction and internal fixation of the fracture. These include:
Kocher approach (fig 3) - In this approach, the radial head is exposed through the interval between the extensor carpi ulnaris and the anconeus. The posterior interosseous nerve (PIN) and the radial nerve must be protected. The posterior fibers of the supinator are incised and the capsule is incised in the mid-radiocapitellar plane anterior to crista supinatoris to avoid damaging the lateral ulna collateral ligament (LUCL). The risk of PIN injury is less than with the Kaplan approach (more posterior). The PIN crosses the proximal radius from anterior to posterior within the supinator muscle 4 cm distal to the radial head. In both Kocher and Kaplan's approach, the forearm should be pronated to protect PIN. The PIN originates approximately 1.2mm from the radiocapitellar joint. Pronation of the forearm pulls the nerve anteriorly and away from the surgical field. There is a risk of destabilizing the elbow if the capsule incision is too posterior and LUCL is cut, which lies below the equator of the capitellum
Kaplan approach (fig 3) - In this approach, the radial head is exposed through the interval between the extensor digitorum communis and extensor carpiradialis bravis. The mid-fibers of the supinator are incised and the capsule is incised anterior to the mid-radiocapitellar plane. There is less risk of disrupting LUCL and destabilizing the elbow than with the Kocher approach. There is improved exposure of the anterior fractured fragments when screw fixation is performed. There, however, is a greater risk of PIN and radial nerve injury and the approach is less extensile.
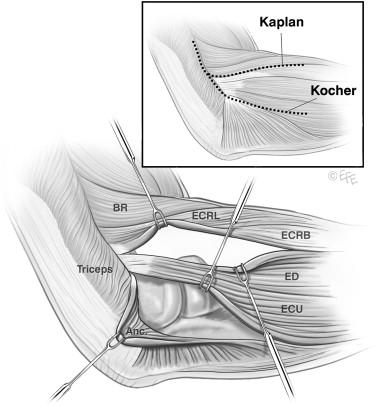
Fig 3- Kaplan and Kocher approach
Extensor digitorum communis (EDC) split - The incision is made longitudinally through the middle of the EDC to the origin on the lateral epicondyle. It provides improved access to the anterior half of the radial head. It also reduces the risk of iatrogenic injury to the lateral collateral ligament complex.
Posterior approach - There is no true intermuscular interval at the posterior aspect of the elbow. A large lateral skin flap is raised to approach the posterior aspect of the elbow. This approach is usually used when there is an associated olecranon or Monteggia fracture. This approach allows access to both the medial and lateral sides of the elbow. This approach is not so popular due to skin flap-related complications.
Technique
Screw(s) - Screws are utilized alone in simple partial articular fractures of the radial head. Herberts headless screws are used to fix articular fracture fragments. Fixation with screws produces better elbow range of motion and functional outcome scores at 1 year compared to plate fixation.
Plates and screws - Plates and screws are used for fractures involving the head and neck of the radius. Mini-fragment (1.5 - 2.0 mm) plates and screws are used to fix the fracture. The plate is placed posterolaterally on the non-articular safe zone that consists of a 90-110º arc defined by the projections of the radial styloid and Lister's tubercle. The bicipital tuberosity is the distal limit of plate placement. Anything distal to that will endanger the PIN. Implants on the articular surface have to be countersunk. Plate removal is relatively common in order to restore forearm rotation.
Complications
Several complications can result from ORIF of radial head fractures. Some of these include:
PIN injury
Destabilization of the lateral ligament complex
Articular surface penetration with screws
Mechanical block to motion by hardware
3. Fragment Excision
If the fracture is less than 25% of the surface area of the radial head and does not compromise elbow stability, the fragment can be excised. A Kocher or Kaplan approach is used for the excision. If the fragment is too large excision can lead to elbow instability.
4. Radial Head Resection
Radial head excision is carried out through the Kocher or Kaplan approach.
Enough radial head should be removed to fully remove comminuted fragments of the radial head and the annular ligament must be kept intact.
Complications following radial head resection include muscle weakness, wrist pain, valgus elbow instability, heterotopic ossification, elbow arthritis,
proximal radial migration, decreased strength, and cubitus valgus.
5. Radial head arthroplasty
There are several types of prostheses for radial head arthroplasty. These include:
1. Metal prostheses - There are 3 types of metal prosthesis:
Loose stemmed prosthesis - They act as a stiff spacer. They are believed to "settle in" to anatomic position throughout the arc of motion.
Press-fit prosthesis - They depend on osteointegration and tight canal fit. They are prone to incorrect intramedullary positioning given their tight fit.
Bipolar prosthesis - They have an articulation at the head-neck junction. They allow better articulation of the radial head to the capitellum throughout the arc of motion. They may cause elbow instability when the radial head angles relative to the radial stem.
2. Pyrocarbon prostheses - Pyrocarbon implants approximate the modulus of cartilage and hence reduce the risk of capitellar wear from the metallic radial head implant. These implants are currently still under investigation.
3. Silicon replacements (Sylastic)- These are no longer used. These replacements are independent risk factor for revision surgery due to
implant fracture and reactive synovitis.
There are 2 types of implant design namely:
Monoblock design where the head and stem are a single connected piece implanted together.
Modular design where the head and stem are 2 distinct pieces that are attached during implantation.
Complications of radial head arthroplasty include:
Radiocapitular overstuffing. Radiocapitular overstuffing can lead to capitellar wear problems and malalignment instability. When the length of the prosthesis is excessive it produces abnormal loads on the capitellum and this produces pain, stiffness, and progressive capitellar erosion. When the diameter of the radial head prosthesis is not correct there is a cam effect that produces abnormal loads through the lateral aspect of the trochlea and the lesser sigmoid notch. Overstuffing is best assessed by direct visualization under fluoroscopy. The proximal part of the implant should align with proximal lesser sigmoid notch and the deepest point of the radial head dish should be at the same level as the lateral coronoid facet. The range of motion should be assessed in flexion and extension and it should be smooth. The radial head should remain properly aligned with the capitellum with elbow extension and flexion as well as with forearm supination and pronation.
Loosening. Loosening is more likely with a press-fit prosthesis. In such situations, there is a higher potential for revision surgery. To prevent loosening the implant may be fixed with bone cement if needed.
Implant dissociation. Implant dissociation can occur with bipolar prosthesis. Metallosis and pain can result when there is a defective locking mechanism of the head on the stem.
Complications from surgical treatment of radial head fractures
1. Surgical Site Infection
The treatment for surgical site infection is incision and drainage. If there is osteomyelitis radial head excision may be necessary. Sometimes the hardware/implant may need removal when infection complicates ORIF or radial head replacement. Intravenous antibiotics are often needed for six weeks followed by oral antibiotics if the hardware/prosthesis is retained.
2. Secondary displacement of the fracture
Secondary displacement occurs in less than 5% of fractures that are initially treated nonoperatively. In such situations, operative fixation may be necessary.
3. Posterior interosseous nerve injury (with operative management)
The risk factors for PIN injury are dissection distal to biceps tuberosity during surgery and overaggressive retraction at the radial neck.
If neuropraxia is suspected, conservative treatment, consisting of a cock-up wrist splint, is carried out. If no recovery occurs after several months of conservative management then an EMG is done. If the nerve palsy is permanent a tendon transfer may be needed.
4. Elbow stiffness & loss of forearm rotation
The incidence of elbow stiffness and loss of forearm movements is between 3% to 20%. The risk factors are prolonged immobilization, intra-articular fracture, malunion, nonunion and heterotopic ossification.
The first line of treatment is non-operative and it includes supervised exercise therapy with static or dynamic progressive elbow splinting over a 6 month period. The primary aim is to achieve "functional" elbow range of motion i.e 100º flexion arc (30º-130º) and 100º of rotation (50º pronation & 50º supination). Sometimes operative treatment is required. There may be a need for release of contracture with or without radial head removal or replacement. Sometimes an anconeus or Achilles allograft interposition arthroplasty is necessary.
5. Radiocapitellar joint arthritis
The risk factors for radiocapitellar arthritis are a fracture with intra-articular displacement and the use of a metallic radial head replacement. The chances of developing arthritis increases with overstuffing.
Nonoperative treatment includes activity modification, anti-inflammatories
medications and injections. Operative treatment includes radial head resection, anconeus or Achilles allograft interposition arthroplasty, and radiocapitellar hemiarthroplasty.
6. Heterotopic ossification (HO)
The risk factors for heterotopic ossification include CNS injury, burns and
elbow fracture/dislocation with significant soft tissue injury. Six weeks of indomethacin can be used to minimize risk after fracture/dislocation. The use of post-operative radiation for prevention and treatment is controversial. Operative removal can be considered after HO is mature. Most patients have satisfactory outcome after excision despite the presence of residual flexion contracture. About 10% of the patients can have a recurrence.
7. Loss of hardware fixation
Loss of hardware fixation can be treated by revision fixation, radial head replacement, or radial head removal.
References
Ring D, Quintero J, Jupiter JB. Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002; 84-A: 1811–1815.
Hildebrand AH, Zhang B, Horner NS, King G, Khan M, Alolabi B. Indications and outcomes of radial head excision: A systematic review. Shoulder Elbow. 2020;12(3):193-202. doi:10.1177/1758573219864305.
Morrey BF, Chao EY, Hui FC. Biomechanical study of the elbow following excision of the radial head. J Bone Joint Surg Am 1979; 61: 63–68.
Fuchs S, Chylarecki C. Do functional deficits result from radial head resection? J Shoulder Elbow Surg 1999; 8: 247–251.
Boulas HJ, Morrey BF. Biomechanical evaluation of the elbow following radial head fracture. Comparison of open reduction and internal fixation vs. excision, silastic replacement, and non-operative management. Chir Main 1998; 17: 314–320.
Karlsson MK, Herbertsson P, Nordqvist A, et al. Long-term outcome of displaced radial neck fractures in adulthood: 16–21 year follow-up of 5 patients treated with radial head excision. Acta Orthop 2009; 80: 368–370.
Postacchini F, Morace GB. Radial head fracture treated by resection. Long-term results. Ital J Orthop Traumatol 1992; 18: 323–330.
Herbertsson P, Hasserius R, Josefsson PO, et al. Mason type IV fractures of the elbow: a 14- to 46-year follow-up study. J Bone Joint Surg Br 2009; 91: 1499–1504.
Iftimie PP, Calmet Garcia J, de Loyola Garcia Forcada I, et al. Resection arthroplasty for radial head fractures: long-term follow-up. J Shoulder Elbow Surg 2011; 20: 45–50.
Coleman DA, Blair WF, Shurr D. Resection of the radial head for fracture of the radial head. Long-term follow-up of seventeen cases. J Bone Joint Surg Am 1987; 69: 385–392.
Faldini C, Nanni M, Leonetti D, et al. Early radial head excision for displaced and comminuted radial head fractures: considerations and concerns at long-term follow-up. J Orthop Trauma 2012; 26: 236–240.
Yalcinkaya M, Bagatur AE, Erdogan S, et al. Resection arthroplasty for Mason type III radial head fractures yield good clinical but poor radiological results in the long term. Orthopedics 2013; 36: e1358–e1364.
Rymaszewski LA, Mackay I, Amis AA, et al. Long-term effects of excision of the radial head in rheumatoid arthritis. J Bone Joint Surg Br 1984; 66: 109–113.
Ikeda M, Sugiyama K, Kang C, et al. Comminuted fractures of the radial head. Comparison of resection and internal fixation. J Bone Joint Surg Am 2005; 87: 76–84.
Ikeda M, Oka Y. Function after early radial head resection for fracture: a retrospective evaluation of 15 patients followed for 3–18 years. Acta Orthop Scand 2000; 71: 191–194.
Ünlü MC, Güven MF, Arslan L, et al. Comparison of the functional results of radial head resection and prosthesis for irreparable mason type-III fracture. Ulus Travma Acil Cerrahi Derg 2018; 24: 359–363.
Burkhart KJ, Mattyasovszky SG, Runkel M, et al. Mid- to long-term results after bipolar radial head arthroplasty. J Shoulder Elbow Surg 2010; 19: 965–972.
Harrington IJ, Sekyi-Otu A, Barrington TW, et al. The functional outcome with metallic radial head implants in the treatment of unstable elbow fractures: a long-term review. J Trauma 2001; 50: 46–52.
Marsh JP, Grewal R, Faber KJ, et al. Radial head fractures treated with modular metallic radial head replacement: outcomes at a mean follow-up of eight years. J Bone Joint Surg Am 2016; 98: 527–535.
Sershon RA, Luchetti TJ, Cohen MS, et al. Radial head replacement with a bipolar system: an average 10-year follow-up. J Shoulder Elbow Surg 2018; 27: e38–e44.
Janssen RP, Vegter J. Resection of the radial head after Mason type-III fractures of the elbow: follow-up at 16 to 30 years. J Bone Joint Surg Br 1998; 80: 231–233.