Patellar Instability
Dr. KS Dhillon
Patella Anatomy
The patella is the largest sesamoid bone in the body. It lies within the quadriceps tendon in front of the knee joint. It originates from multiple ossification centers that appear from the ages of three to six, and they coalesce rapidly. It's a thick, flat, triangular bone with its apex pointing downwards and the base lies proximally. It has a medial and lateral border.
The patella is a dense trabecular bone with a thin compact lamina covering it. The quadriceps muscle is attached on the superior surface and extends distally onto the anterior surface. The vastus lateralis is attached on the lateral and the vastus medialis on the medial border. At the apex, the patella ligament is attached. The ligament inserts onto the tibial tuberosity on the anterior surface of the tibia.
The patella is stabilized by the horizontal fibers of the vastus medialis, the medial patella retinaculum as well as the anterior projection of the lateral femoral condyle.
The blood supply to the patella arises from the genicular arteries which are branches of the popliteal artery. They form a peripatellar anastomosis and supply blood to the patella and the knee joint.
The superior two-thirds of the posterior articular surface of the patella articulates with the anterior surface of the femoral condyles. The lateral articular surface of the patella is usually larger than the medial articular surface. However, the medial femoral condyle is larger and projects further anteriorly than the lateral femoral condyle.
Patellar instability
Patellar instability is a condition characterized by episodes of patellar subluxation or dislocation as a result of injury, ligamentous laxity, or increased Q angle of the knee.
The diagnosis is made clinically in the acute setting with a patellar dislocation with a traumatic knee effusion. In the chronic setting, the diagnosis is made with passive patellar translation and a positive J sign. The J-sign refers to the inverted ‘J’ track the patella takes from extension to early flexion (or vice versa) in a maltracking patella. The laterally subluxated patella suddenly shifts medially as it engages the trochlear groove of the distal femur. The J-sign on clinical examination is suggestive of patellar maltracking and potential instability.
The initial treatment is nonoperative with bracing for first-time dislocation without bony avulsion or the presence of articular loose bodies. Operative treatment is indicated for chronic and recurrent patellar instability.
Epidemiology
Patella dislocations account for about 3% of all knee injuries. The majority of injuries occur in young individuals. Most patients with patellar instability are aged between 10 years to 16 years and are females. The incidence of patellar instability in the general population is about 5.8 per 100,000 and about 29 per 100,000 in the 10 to 17-year-old age group.
The risk factors for patellar instability include:
1. Ligament laxity (Ehlers-Danlos syndrome)
2. Previous episode of patellar instability
3. Malalignment syndrome that leads to an increased Q angle due to
femoral anteversion, genu valgum, and external tibial torsion.
4. Patella alta
5. Trochlear dysplasia
6. Excessive lateral patellar tilt
7. Lateral femoral condyle hypoplasia
8. Dysplastic vastus medialis oblique (VMO) muscle
9. Overpull of lateral structures i.e iliotibial band and vastus lateralis
Etiology
Patella dislocation is usually due to a noncontact twisting injury with the knee extended and the foot externally rotated. The patient will usually reflexly contract the quadriceps and the patella reduces itself. Osteochondral fractures can occur when the patella relocates. A direct blow is a less common cause of dislocation. It can be due to knee to knee collision in basketball or football helmet to side of the knee.
Patellar instability classification
Patellar instability can be classified as follows:
1. Acute traumatic
Occurs equally in males and females. It may occur from a direct blow.
2. Chronic pathological laxity of the patella
There are recurrent episodes of patella subluxation. It occurs more often in females. It is associated with malalignment of the patella.
3. Habitual
It is usually painless. It occurs during knee flexion. The pathology is usually proximal i.e tight iliotibial band and vastus lateralis.
Clinical Presentation
The patient usually presents with anterior knee pain and complains of instability of the affected knee.
In patients with acute dislocation, examination reveals a large hemarthrosis
and medial patellofemoral joint tenderness. There is an increase in passive patellar translation. Lateral translation of the medial border of the patella to the lateral edge of the trochlear groove is considered as abnormal amount of translation. There will be patella apprehension. Passive lateral translation of the patella results in guarding and a sense of apprehension. The Q angle will be increased. The J sign is present where the patella with excessive lateral translation in extension "pops" into the groove as the patella engages the trochlea early with knee flexion. Often there is patella alta.
Imaging
Plain radiographs will help to rule out fractures or loose bodies. The fracture is usually seen at the medial patellar facet (most common) and the lateral femoral condyle. The AP views are the best to evaluate overall lower extremity alignment. The lateral views are the best to assess trochlear dysplasia. A crossing sign represents a flattened trochlear groove where the trochlear groove lies in the same plane as the anterior border of the lateral condyle.
A double contour sign represents a convex trochlear groove/hypoplastic medial condyle where the anterior border of the lateral condyle lies anterior to the anterior border of the medial condyle. A supratrochlear spur may be present. It arises in the proximal aspect of the trochlea (fig 1).

Fig 1.
The lateral views are also used to evaluate patellar height (patella alta vs. patella baja).
In a lateral x-ray taken at 30 degrees of knee flexion a line drawn through the roof [dome] of the intercondylar notch (Blumensaat's line), should intersect the lower pole of the patella. If the patella is above this line, it is called patella alta or high patella.
Multiple ratios can be calculated to get an idea about the level of the patella.
1. Insall-Salvati ratio (normal 0.8 - 1.2)
It is the ratio of the patellar tendon length to the length of the patella.
If the ratio is more than 1.2, it indicates a Patella Alta. If less than 0.8 it indicates patella baja.
2. Blackburn-Peel ratio (normal 0.5-1)
It is the ratio of the perpendicular distance between the tibial plateau and patellar articular surface to the length of the patella articular surface. A ratio of more than 1 indicates Patella Alta.
3. Caton-Deschamps - (normal 0.6-1.3)
It is the ratio of the distance between the most inferior point of the patella articular surface to the anterior angle of the tibial plateau and the length of the patellar articular surface. A ratio of more than 1.3 indicates Patella Alta.
Sunrise/merchant views are done to assess patellar tilt. The lateral patellofemoral angle (LPFA), as described by Laurin, is the angle between the line parallel to the tip of the anterior condyles and the lateral patellar facet. The normal angle is more than 11 degrees opening laterally. It measures tilt with subluxation.
The congruence angle is an index of patella subluxation. It is measured from a line through the apex of the patella to a line bisecting the trochlea.
If the congruence angle is lateral to the congruence line, it is considered positive. If the congruence angle is medial to the congruence line, it is considered negative. The normal angle is less than -6 meaning the more positive the angle, the more subluxed the patella is laterally. The angle is abnormal if it is greater than 16°, indicating patellar subluxation (fig 2).
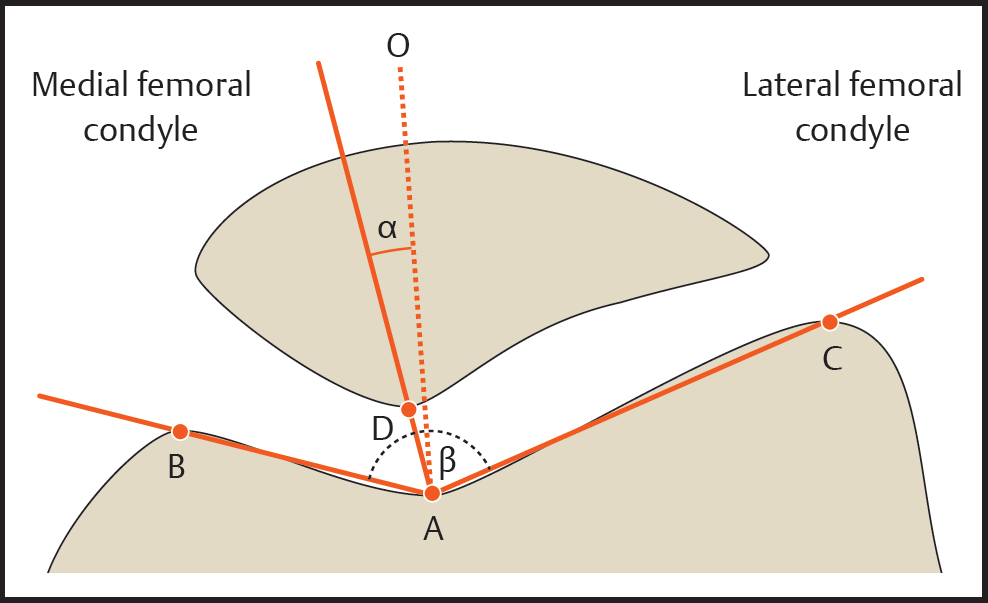
Fig 2
CT scan
Tibial tuberosity-trochlear groove (TT-TG) distance is a measure of lateralization of the tibial tuberosity in relation to the femoral trochlea.
The TT-TG distance represents the radiographic measurement of the quadriceps vector, which represents a lateral force displacement on the patella during knee motion. A line is drawn through the deepest point of the trochlear groove, perpendicular to the posterior femoral condylar tangent (TT). A second line is drawn in parallel to the trochlear line through the most anterior portion of the tibial tubercle (TG). The distance between the 2 lines represented the TT-TG distance.
It is more than 20 mm in patients with recurrent patellar dislocations, as compared with 13 mm in control subjects (Fig 3).
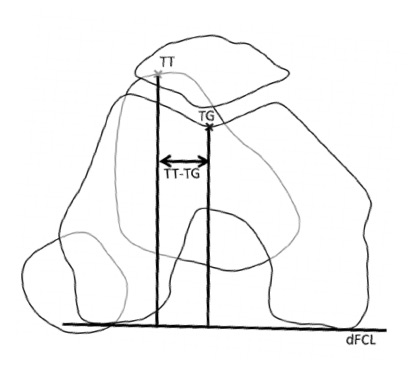
Fig 3.
MRI
It is useful for evaluating loose bodies and assessing the medial patellofemoral ligament (MPFL). Osteochondral lesion and/or bone bruising is commonly seen on the medial patellar facet and the lateral femoral condyle. Tears of the MPFL are usually seen at the medial femoral epicondyle.
Treatment in Adults
Nonoperative
For acute dislocation, a closed reduction is carried out. In majority of patients, spontaneous reduction occurs. The treatment includes the use of NSAIDs, activity modification, and physical therapy.
The indications for non-operative treatment include:
First-time dislocation
No loose bodies or articular damage
No osteochondral fragments
Habitual dislocators
Patients with connective tissue disease - Ehlers Danlos
Physical therapy focuses on closed chain exercises and quadriceps strengthening exercises. Core hip strengthening and gluteal muscle strengthening helps to improve external rotators of the hip, thus externally rotating the femur and decreasing the Q-angle.
Patellar stabilizing sleeve or "J" brace can be used and patella taping can be carried out. Knee aspiration is carried out if there is tense effusion.
Operative Treatment
The indications for operative treatment include:
Osteochondral injury with loose body
Chronic instability
Failure of nonsurgical treatment
Arthroscopic debridement with removal of loose bodies is done if there are loose bodies or osteochondral damage is seen on imaging. Open reduction internal fixation with screws and pins is carried out if there is sufficient bone available for fixation.
Direct repair of the MPFL can be carried out when there is an acute first-time dislocation with a bony fragment.
MPFL reconstruction with autograft or allograft can be carried out when there is recurrent instability and no malalignment or trochlear dysplasia. Gracillis or semitendinosus is commonly used. The femoral origin can be reliably found (Schottles point). The Schottle point is 1 mm anterior to the posterior cortex line, 2.5 mm distal to the posterior origin of the medial femoral condyle, and proximal to the posterior point of the Blumensaats line. Tensioning of the graft should be done between 60 to 90 degrees of knee flexion. Severe trochlear dysplasia is the most important predictor of residual patellofemoral instability after isolated MPFL reconstruction.
When there is significant malalignment a Fulkerson-type osteotomy is carried out in isolation or in combination with MPFL reconstruction. The osteotomy involves anterior and medial, tibial tubercle transfer with fixation. It is carried out if TT-TG is more than 20mm. It decreases pressure on the lateral patellar facet and trochlea.
Lateral release of the patella has been shown to be ineffective for the treatment of patellar instability. It is used for lateral compression syndrome where there is combined or isolated patellar tilt or excessive tightness after medialization procedure.Usually, the lateral release is combined with a medialization procedure and not done in isolation.
Trochleoplasty to deepen the sulcus of the distal femoral trochlea has limited use due to serious irreversible articular and subchondral injury to the trochlea. It is indicated for abnormal patellar tracking with J sign caused by femoral trochlear dysplasia. The cancellous bone is exposed in the trochlea, and a strip of cortical bone on the edge of the trochlea is elevated. A new trochlea sulcus is created, and the trochlear bone shell is impacted and secured to the new sulcus fixed with staples or sutures.
Pediatric treatment
The principles of treatment in children are the same as in adults, except that the physis must be preserved in children. A tibial tubercle osteotomy should not be done since it will harm the growth plate of proximal tibia.
Recurrent dislocation rates with nonoperative treatment may be as high as 15-50% at 2-5 years. Recurrence rate is highest in patients who sustain a primary dislocation before the age of 20 years.
Medial patellar dislocation and medial patellofemoral arthritis can occur as a result of prior patellar stabilization surgery.