Phocomelia
Dr. KS Dhillon
Introduction
Phocomelia (fig 1) is a rare congenital disorder. It is defined by the absence of intermediate segments of the extremity. In children with phocomelia, the hands or feet are directly attached to the trunk. Phocomelia is a teratogenic side effect of the drug thalidomide. This drug was first marketed to treat anxiety and morning sickness. There were claims that the drug was safe during pregnancy. It was however removed from the market in the 1960s when doctors noted an association with phocomelia. About 40% of patients affected by the teratogenic effects of thalidomide die near the time of birth. These congenital disabilities had a profound political and social impact on drug regulation and proof of safety (1,2).
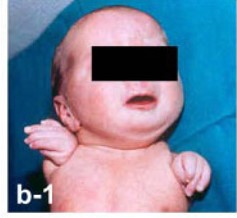
Fig 1.
Etiology
Phocomelia is the most notable side effect of thalidomide. In the last 30 years, there have been several cases of phocomelia associated with thalidomide use. Today however the cause of most cases is undetermined. Despite strict regulation worldwide, there have been several cases of phocomelia attributed to thalidomide. Underdeveloped countries and those that are endemic with leprosy where thalidomide remains in use, still report cases of defects caused by thalidomide exposures in pregnancy. In more developed countries with strict regulations, there has been a dramatic decrease in the incidence of phocomelia within the general population (3,4).
Besides the teratogenicity of thalidomide, researchers have hypothesized that phocomelia is associated with anomalous origins of the subclavian artery. This results in a disrupted vascular supply to intermediate limb segments (5,6).
Epidemiology
Bermejo-Sanchez et al (1) examined 22,740,933 live births to study the incidence and presentation of phocomelia to assess the prevalence of true phocomelia. According to reports true phocomelia occurs in 0.62 live births per every 100,000 births. About half (53.2%) of the cases displayed isolated phocomelia, 36.9% had additional major congenital abnormalities, and 9.9% of cases correlated with a clinical syndrome.
According to the data one limb was involved in 55.9% of the cases, while in 40.2% of cases, two limbs were involved. Of the 141 cases, only four cases had involvement of all four limbs. When single upper limb deficiencies are compared, the left side is more commonly affected (64.9%) than the right side. When two limbs are involved, the upper limbs are involved 58.5% of the time compared to the lower limbs (1,7).
Pathophysiology
When the extremity develops, the apical ectodermal ridge forms at the most distal end of the limb bud. This apical ectodermal ridge, through its interaction with the underlying progress zone mesoderm, determines the appropriate longitudinal growth of the extremity and differentiation of the limb bud's distal and proximal structures. Cell death due to apoptosis from any cause such as drug toxicity or vascular insufficiency that interrupts this relationship between the apical ectodermal ridge and the progress zone can produce phocomelia (8).
History and Physical Examination
Whenever phocomelia is identified in a newborn, given its correlation with thalidomide, doctors should inquire about medications taken during early pregnancy. Children with phocomelia should undergo a thorough physical examination since one study reported that 36.9% of phocomelia cases have additional major malformations, with 9.9% of cases being attributable to various syndromes (1).
Evaluation
In children when phocomelia is identified, the doctors should complete a thorough search for other associated abnormalities. Other defects are present in approximately half of the patients with this limb anomaly. Doctors should examine the musculoskeletal system, including the heart, vertebrae, and intestines, as dysfunction in these organ systems appears most frequently in conjunction with phocomelia (1).
Management
In the management of children born with phocomelia, it is important to look for other associated abnormalities, especially of the intestines and heart, and address them promptly. Gastroenterologists and pediatric cardiologists should examine the child and recommend a treatment plan for abnormalities encountered.
For patients with hypoplastic limbs, prosthetics may be of some value. Many without concomitant pathology can function quite well. Families of children with severely hypoplastic extremities should work with therapists to meet the unique needs of their children. Caring for a disabled child can be traumatic for some people. Hence, physicians should have a low threshold to recommend mental counseling services to assist in coping mechanisms that may be needed by both the child and the parents.
Differential Diagnosis
Bermejo-Sanchez et al (1) reported that 9.9% of cases of phocomelia are associated with different syndromes. They are listed here in order of decreasing prevalence:
Roberts Syndrome: A rare autosomal recessive disorder caused by a mutation in the ESCO2 gene that manifests with severe limb malformations and craniofacial defects (9).
Thrombocytopenia with radial aplasia (TAR): A rare autosomal recessive disorder related to the RBM8A gene that presents with thrombocytopenia and limb radial deficiency (10).
Syndrome of severe limb defects, vertebral hypersegmentation, and mirror polydactyly: An autosomal recessive disorder resulting in severe limb hypoplasia with polydactyly and hypersegmentation of the spine (11).
Prognosis
In a review study by Bermejo-Sánchez, there were 85 live births to every 24 stillbirths for children with phocomelia. In patients with isolated phocomelia, there were 57 live births to every eight stillbirths (1).
Complications
Children with phocomelia have a higher stillbirth rate as compared to the general population. Children with severe limb hypoplasia may face problems with mobility and activities of daily life.
Patient Education
The incidence of thalidomide-induced limb hypoplasia has significantly reduced due to increased drug regulatory practices across the world. Thalidomide can be used for the treatment of insomnia, anxiety, and even leprosy. It is important to understand the risks of thalidomide exposure during pregnancy for any woman taking the medication. Patients and doctors should understand the deleterious effects of thalidomide when taken in early pregnancy.
Conclusion
In the regulatory practices of pharmacology, phocomelia and the thalidomide controversy were critical steps forward. The most important responsibility of the healthcare community with regards to phocomelia, is the prevention of prescribing unsafe medications that can cause limb truncation. This can be done through careful prescribing practices and patient education.
For patients born with limb hypoplasia, including phocomelia, an interdisciplinary team of specialists needs to examine the patient. This team can screen patients for associated abnormalities that may be fatal since half of the patients with phocomelia and amelia have associated defects. Many related abnormalities of the vertebrae, heart, or other vital organs may be life-threatening. These anomalies should be addressed promptly by the physicians. If surgical intervention is required, the dedicated OR team must be well-versed with the operative plan and work efficiently to optimize patient outcomes.
A prosthetist and therapist can help a developing child with disabilities to function at a higher level. Families of these disabled children are often under tremendous financial and emotional strain. Hence, appropriate mental health counseling and social work may be necessary to care for the patient and their families.
References
Bermejo-Sánchez E, Cuevas L, Amar E, Bianca S, Bianchi F, Botto LD, Canfield MA, Castilla EE, Clementi M, Cocchi G, Landau D, Leoncini E, Li Z, Lowry RB, Mastroiacovo P, Mutchinick OM, Rissmann A, Ritvanen A, Scarano G, Siffel C, Szabova E, Martínez-Frías ML. Phocomelia: a worldwide descriptive epidemiologic study in a large series of cases from the International Clearinghouse for Birth Defects Surveillance and Research, and overview of the literature. Am J Med Genet C Semin Med Genet. 2011 Nov 15;157C(4):305-20.
Ridings JE. The thalidomide disaster, lessons from the past. Methods Mol Biol. 2013;947:575-86.
Castilla EE, Ashton-Prolla P, Barreda-Mejia E, Brunoni D, Cavalcanti DP, Correa-Neto J, Delgadillo JL, Dutra MG, Felix T, Giraldo A, Juarez N, Lopez-Camelo JS, Nazer J, Orioli IM, Paz JE, Pessoto MA, Pina-Neto JM, Quadrelli R, Rittler M, Rueda S, Saltos M, Sánchez O, Schüler L. Thalidomide, a current teratogen in South America. Teratology. 1996 Dec;54(6):273-7.
Schuler-Faccini L, Soares RC, de Sousa AC, Maximino C, Luna E, Schwartz IV, Waldman C, Castilla EE. New cases of thalidomide embryopathy in Brazil. Birth Defects Res A Clin Mol Teratol. 2007 Sep;79(9):671-2.
van der Horst RL, Gotsman MS. Anomalous origin of the subclavian artery associated with phocomelia. S Afr Med J. 1971 Dec 18;45(48):1397-9.
Bavinck JN, Weaver DD. Subclavian artery supply disruption sequence: hypothesis of a vascular etiology for Poland, Klippel-Feil, and Möbius anomalies. Am J Med Genet. 1986 Apr;23(4):903-18.
Källén B, Rahmani TM, Winberg J. Infants with congenital limb reduction registered in the Swedish Register of Congenital Malformations. Teratology. 1984 Feb;29(1):73-85.
Knobloch J, Rüther U. Shedding light on an old mystery: thalidomide suppresses survival pathways to induce limb defects. Cell Cycle. 2008 May 01;7(9):1121-7.
Ismail S, Essawi M, Sedky N, Hassan H, Fayez A, Helmy N, Shehab M, Farouk D, Elruby M, Otaify G, Eldarsh A, Hosny L, Gaber K, Aboul-Ezz EHA, Ramzy MI, Mehrez MI, Hassib NF, Elhadidi SMA, Aglan MS, Temtamy SA. ROBERTS SYNDROME: CLINICAL AND CYTOGENETIC STUDIES IN 8 EGYPTIAN PATIENTS AND MOLECULAR STUDIES IN 4 PATIENTS WITH GENOTYPE/PHENOTYPE CORRELATION. Genet Couns. 2016;27(3):305-323.
Al-Qattan MM. The Pathogenesis of Radial Ray Deficiency in Thrombocytopenia-Absent Radius (TAR) Syndrome. J Coll Physicians Surg Pak. 2016 Nov;26(11):912-916.
Urioste M, Lorda-Sánchez I, Blanco M, Burón E, Aparicio P, Martínez-Frías ML. Severe congenital limb deficiencies, vertebral hypersegmentation, absent thymus and mirror polydactyly: a defect expression of a developmental control gene? Hum Genet. 1996 Feb;97(2):214-7.