Trigger Finger
DR KS Dhillon
Introduction
Trigger finger (TF) is one of the most common upper limb problems. It is the most common cause of hand pain and disability. It is caused by thickening of the flexor tendon within the distal aspect of the palm [1,2]. This thickening causes abnormal gliding of the tendon within the tendon sheath. The affected tendon gets caught at the edge of the first annular (A1) pulley.
Patients can have difficulty flexing the affected digit if the tendon is caught distal to the A1 pulley. They can have difficulty in extending the digit if the tendon is caught proximal to the pulley. The condition can be very painful, especially when the locked digit snaps or releases beyond the restriction by the use of increased force.
The etiology of TF remains unknown. Triggering occurs more frequently in patients with diabetes mellitus (DM) and those with rheumatoid arthritis (RA).
In the beginning patients with TF have discomfort in the palm during movements of the involved digit. Gradually or, in some cases acutely, the flexor tendon causes painful snapping or popping as the patient flexes and extends the digit. The patient often presents with a digit locked in a particular position, most often flexion, which requires gentle, passive manipulation into full extension [3].
TF has a predilection for the dominant hand. The most commonly affected digit is the thumb, followed by the ring, middle, little, and index finger. A retrospective study by Schubert et al [4] of 577 TFs, however, found no relation to hand dominance. The involvement of more than one finger is not unusual.
Trigger finger occurs mostly in the adult population and much less frequently in the pediatric population. Most frequently it occurs in the thumb [5]. The condition in children has been referred to as congenital trigger thumb [6]. Evidence, however, indicates that it usually presents sometime after infancy and is thus more appropriately referred to as pediatric trigger thumb [7].
In the past, triggering of the digits was treated by splinting in extension. This caused stiffness and, consequently, loss of MCP and IP flexion. Because of dissatisfaction with this form of treatment, researchers used intrasheath steroid injections instead. This resulted in a high proportion of good outcomes [4,8].
The first line of treatment for trigger digit is steroid injection with surgical release of the A1 pulley as the second line of treatment.
Anatomy
Fingers
Tendon sheaths of the long flexors run from the level of the metacarpal heads to the distal phalanges. They are attached to the underlying bones and volar plates. This will prevent the tendons from bowstringing. Thickenings in the fibrous flexor sheath act as pulleys that direct the sliding movements of the fingers (fig 1).
There are two types of pulleys i.e. the annular (A) and cruciate (C) pulleys. Annular pulleys are composed of single fibrous bands, whereas the cruciate pulleys have two crossing fibrous bands.
The order of the pulleys from proximal to distal is as follows:
The A1 pulley overlies the MCP joints; it is released during surgery for TF. The A2 pulley overlies the proximal end of the proximal phalanx
The C1 pulley overlies the middle of the proximal phalanx
The A3 pulley lies over the PIP joint
The C2 pulley lies over the proximal end of the middle phalanx
The A4 pulley lies over the middle of the middle phalanx
The C3 pulley lies over the distal end of the middle phalanx
The A5 pulley lies over the proximal end of the distal phalanx
The A2 and A4 pulleys are vital in preventing bowstringing of the flexor tendons. They have to be preserved or reconstructed after any damage to them.
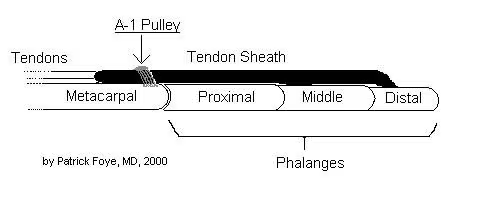
Fig 1.
Thumb
The flexor anatomy of the thumb is different from that of the fingers. The flexor pollicis longus (FPL) tendon is a single tendon within the flexor sheath. It inserts onto the base of the distal phalanx. The fibro-osseous sheath is composed of two annular pulleys (A1 and A2) that arise from the palmar plates of the MCP and IP joints respectively. The oblique pulley, which originates from and inserts onto the proximal phalanx, is the most important pulley. It is approximately 10 mm in length. It blends with a portion of the adductor pollicis insertion.
The digital nerves and arteries run parallel to the tendon sheath. At the level of the MCP flexion crease, they lie just under the skin. Proximal to the A1 pulley, the radial digital nerve of the thumb crosses obliquely over the tendon sheath.
Pathophysiology
In most cases of trigger finger there is a mismatch between the flexor tendon and the proximal pulley mechanism. The finger flexor tendons normally glide back and forth under a restraining pulley [9,10,11].
Thickening of the flexor tendon sheath restricts the normal gliding movements. A nodule can develop on the tendon, causing the tendon to get stuck at the proximal edge of the A1 pulley when the patient is attempting to extend the digit.
When forceful attempts are made to extend the digit, by using increased force from the finger extensors or by applying an external force, the digit classically snaps open with significant pain. Less commonly, the nodule is present distal to the A1 pulley. This results in difficulty flexing the digit.
There is a newer technique for quantitative assessment of the stiffness of soft tissues called sonoelastography. A study by Miyamoto et al [12] noted that the causes for snapping in TF were increased stiffness and thickening of the A1 pulley. Three weeks after corticosteroid injection, the pulley thickness and the ratio of subcutaneous fat to the pulley both decreased. With the injection snapping disappeared in all patients studied.
Etiology
The etiology of trigger finger remains unknown. It is believed that nodule formation in the tendon, morphologic changes in the pulley, or both in combination may affect triggering. Why these changes are initiated remains unknown.
There are several studies that have demonstrated a correlation between TF and activities that require exertion of pressure in the palm while a powerful grip is used or that involve repetitive, forceful digital flexion. Proximal phalangeal flexion in power-grip activities produces high annular loads at the distal edge of the A1 pulley. Hueston and Wilson [13] have suggested that bunching of the interwoven tendon fibers causes the reactive intratendinous nodule that is observed at surgery.
Although the exact etiology remains unknown, there are certain conditions such as DM or RA that can predispose an individual to triggering of the digit.
Sampson et al [14] were of the opinion that the underlying pathobiologic mechanism for triggering is fibrocartilaginous metaplasia of the pulleys due to trauma or disease. There are several studies that have failed to demonstrate the presence of acute or chronic inflammatory cells within the tenosynovium. The exact etiology is unknown, but DM or autoimmune diseases can contribute to morphologic changes in the pulley and/or the tendon sheath to cause triggering. Systemic causes of TF are collagen-vascular diseases which include the following [15] :
Psoriatic arthritis
Amyloidosis
RA
DM
Hypothyroidism
Sarcoidosis
Pigmented villonodular synovitis
Septic causes of TF are secondary infections such as tuberculosis. A few case reports have documented rare causes of TF, including tenosynovitis that resulted from a Mycobacterium kansasii infection in an immunocompetent patient.
There have been suggestions for a long time that there is an association of idiopathic TF with idiopathic carpal tunnel syndrome. There was a study of 551 patients with no predisposing causes diagnosed with either TF, carpal tunnel syndrome, or both based on clinical examination. The study reported that 43% of patients with TF also had concomitant carpal tunnel syndrome. This is significantly higher than the population prevalence of carpal tunnel syndrome, which is about 4% [16].
A study by Grandizio et al [17] showed that the risk of developing TF following carpal tunnel release is greater in patients with DM than in those without DM. The investigators found that out of the 1003 carpal tunnel releases in patients without DM, the incidence of TF at 6 and 12 months was 3% and 4%, respectively. Out of 214 carpal tunnel releases in patients with DM, the incidence of TF at 6 and 12 months was 8% and 10%, respectively. The severity of the DM was not a significant factor in the development of TF.
Trigger thumb
Trigger thumb usually develops idiopathically. It develops more frequently in individuals with osteoarthritis or diabetes. Trigger thumb often develops in individuals with any condition that causes diffuse proliferation of the tenosynovium, such as gout, inflammatory arthritis, or chronic infection such as fungus, or atypical mycobacteria. The diffuse proliferation can extend distally to the MCP joint and, when severe, can cause stiffness rather than intermittent triggering. Some people are more prone to tenosynovitic conditions. Patients with trigger thumb are more likely to develop carpal tunnel syndrome and de Quervain disease. The roles of overuse and trauma in trigger thumb are controversial. Trigger thumb does have a predilection for the dominant hand.
Epidemiology
Trigger finger is a relatively common condition. It occurs two to six times more frequently in women as compared to men. The peak incidence of trigger finger is in individuals aged 55-60 years. TF in children occurs much less frequently than in adults and develops almost exclusively in the thumb [5].
Prognosis
Injection with or without splinting
The prognosis for trigger finger is very good. Most patients respond to corticosteroid injections. Some cases of TF can resolve spontaneously and then reoccur.
Freiberg et al [18] found a greater success rate for TF injection therapy when it was used in patients in whom an examiner could palpate a discrete nodular consistency in the flexor sheath. Digits with a discrete, palpable nodule had a 93% success rate with a single injection of triamcinolone at 3 months follow-up. Digits with a diffuse pattern had a 52% failure rate.
Marks and Gunther [8] reported an 84% success rate in trigger fingers and a 92% success rate in trigger thumbs following an injection of triamcinolone.
Miyamoto et al [12] by using sonoelastography for quantitative assessment of the stiffness of soft tissues, noted that the causes for snapping in TF were increased stiffness and thickening of the A1 pulley. Three weeks after corticosteroid injection, the pulley thickness and the ratio of subcutaneous fat at the pulley both decreased and snapping disappeared in all patients.
Griggs et al [19] reported a success rate of 50% for steroid injections in patients with DM. Patients with insulin-dependent diabetes had a higher incidence of multiple-digit involvement. They required surgical release more frequently than did patients who were not insulin-dependent [20,21].
Surgery
The outcome of surgical release is generally very good. Percutaneous trigger finger release has been reported to be safe and efficacious, with success rates of 74-94%. No complications have been found at medium-term follow-up. The procedure is carried out in individuals with established primary TF who have symptoms lasting longer than 4 months as well as for patients in whom injection therapy has failed to relieve symptoms. It is considered a reasonable choice following one injection failure.
The prognosis for congenital trigger thumb that is treated with resection of the tendon nodule is also very good.
A study by Moriya et al [22] showed that the perioperative characteristics and outcomes differ between TF and trigger thumb and that the surgical outcome is poorer for TF than for trigger thumb. This is partly due to flexion contracture of the PIP joint of the finger.
Pediatric
Triggering can resolve spontaneously in 23-63% of pediatric cases. If children are not treated by the time they have reached the age of 4 years, some may be left with permanent flexion contractures. Surgical release of the A1 pulley before this age leads to excellent results [23,24,25].
History
Some of the patients with trigger finger may have a history of diabetes mellitus or rheumatoid arthritis. In such individuals, multiple digits may be involved.
Some of the patients will give a history of repetitive trauma to the affected area. Other patients may have jobs that require repetitive use of the involved tendons [26].
Signs and symptoms of TF include the following:
Locking or catching during active flexion-extension activity
Stiff digit, especially in neglected or long-standing
Pain over the distal palm
Pain radiating along the digit
Palpable nodule in the line of the flexor digitorum superficialis, just distal to the metacarpophalangeal joint in the palm
Fixed-flexion deformity in the proximal interphalangeal (PIP) joint in late presentations
Triggering on active or passive extension of the digit by the patient
Palpable snapping sensation or crepitus over the A1 pulley
Tenderness over the A1 pulley
Evidence of associated conditions such as gout and rheumatoid arthritis
Early signs of triggering in other digits The triggering may be bilateral
A classic complaint is difficulty in achieving full extension of a single digit, that eventually releases or snaps open with pain at the distal palm and into the digit.
Some patients have difficulty with finger flexion rather than extension. Other patients may have a painful nodule in the distal palm without any triggering or catching.
Some patients report stiffness in the fingers, especially after they have been asleep or following periods of inactivity.
Some of the patients report swelling of the affected digit, especially at the digit's base or proximal aspect.
Pediatric
Children who have trigger thumb rarely complain of pain. These children are usually brought in for evaluation when aged 1-4 years when the parent notices a flexed posture of the thumb’s interphalangeal joint. They often have bilateral fixed flexion contractures of the thumb by the time they present to the physician [27].
Physical Examination
At the level of the distal palmar crease overlying the MCP joint, a tender nodule can usually be palpated.
The affected digit may lock in a flexed position or less often in the extended position. There can be snapping or triggering when the patient attempts to move the digit more forcefully beyond the restriction. The triggering movement is usually very painful. In severe cases, the patient is unable to move the digit beyond the restriction.
In patients with a trigger thumb, the tenderness is found at the palmar aspect of the first MCP joint rather than over the distal palmar crease.
Diagnostic Considerations
The following clinical situations can simulate the locking seen in trigger finger:
Collateral ligaments of the metacarpophalangeal joint catch on a bony prominence such as osteophyte on the side of the metatarsal head.
A partially lacerated flexor tendon catches against the A1 pulley or the FDS decussation.
A nodule in the FDS catches against the A3 pulley.
Locking is simulated by abnormal sesamoids.
Localized swelling in the flexor digitorum profundus gets entrapped at the decussation of the flexor digitorum superficialis (FDS).
A loose body is present in the MCP joint.
Snapping or subluxation of the extensor digitorum communis (EDC) occurs.
Other problems to consider in patients who may have TF include the following:
Ganglion involving the tendon sheath.
Ganglion cyst of the wrist.
Infection within the tendon sheaths.
Acromegaly - Increased growth hormone stimulates sodium reabsorption in the distal nephron. This increases the extracellular volume leading to swelling of the flexor synovium within the digital sheath [22].
The most important differential diagnosis is infection, such as suppurative tenosynovitis. Any such infection requires immediate treatment.
Differential Diagnoses
The differential diagnosis includes:
Dupuytren Contracture
Carpal Tunnel Syndrome
Rheumatoid Arthritis (RA)
Type 1 Diabetes Mellitus
Workup
The diagnosis of trigger finger (TF) is clinical. Occasionally, the nodule in the tendon is easily felt. A palpable and audible click can be appreciated when the triggering is relieved with forced extension of the digit.
No lab tests are needed for the diagnosis of TF. For associated conditions, such as diabetes mellitus (DM), rheumatoid arthritis (RA), or another connective tissue disease, tests such as those assessing glycosylated hemoglobin (HbA1c), fasting blood sugar, or rheumatoid factor (RF) can be done.
Radiography
Radiographs are rarely needed for the diagnosis of TF [28]. Hand radiographs are done if abnormal pathology such as abnormal sesamoids, loose bodies in the metacarpophalangeal [MCP] joint, osteoarthritic spurs on the metacarpal head, or avulsion injuries of collateral ligaments is suspected.
Radiographs are useful to exclude fracture malunion, osteoarthritis, foreign body, or a large sesamoid bone that is affecting interphalangeal joint motion.
Histologic Findings
In patients with TF, the A1 pulley exhibits a marked degree of hypertrophy, described as a white, cicatricial, collarlike thickening. Microscopy demonstrates cyst formation, degeneration, and plasma-cell infiltration. Microscopic studies also show chondrocytic proliferation of type III collagen instead of chondrocyte presence in the normal innermost or friction layer of the A1 pulley [29]. The amount of extracellular matrix is significantly increased when compared with controls.
Staging
Green's classification of triggering is used for clinical grading and documentation. There is no correlation between the grading and the outcome following injection therapy. The grades are defined as follows
[30]:
Grade I (pretriggering) - There is pain and a history of catching that is not demonstrable on clinical examination. There is tenderness over the A1 pulley.
Grade II (active) - There is demonstrable catching but with the ability to actively extend the digit.
Grade III (passive) - There is demonstrable locking in which passive extension is required (grade IIIA) or where the patient is unable to actively flex (grade IIIB).
Grade IV (contracture) - There is demonstrable catching, with a fixed flexion contracture of the proximal interphalangeal joint.
Management
The earlier series recommended surgical treatment for trigger finger as straightforward and highly effective, while regarding prolonged conservative treatment as expensive and unreliable. Subsequent series, however, showed poor results from surgical treatment in 7-9% of cases.
Lapidus in 1972, reversed his previous recommendation for operative treatment of TF after he and Guidotti reported uniformly good results with a single injection of prednisolone into the tendon sheath [31]. Later, Rhoades et al [32] reported a 72% success rate in a series of 53 digits following injection and immobilization.
Injection therapy is now the first line of management. Surgery is done in patients in whom injection treatment has failed. Surgery is also done in individuals who have other pathology, particularly rheumatoid arthritis (RA), which is suspected to be causing triggering that cannot be treated conservatively [33]. There are no absolute contraindications for surgical treatment.
The European HANDGUIDE Group, in May 2014, published a guideline for the multidisciplinary treatment of trigger fingers [34]. By consensus, suitable treatment options included the following:
Orthoses (splinting)
Corticosteroid injections
Corticosteroid injections plus the use of orthoses
Surgery
The severity and duration of the disease and prior treatments received are the primary factors that influence the choice of therapy [34].
Conservative treatment
In adults, most trigger digits can be managed successfully with local steroid injections and splinting [35]. Topical or oral pharmacologic measures are also effective. According to a 2021 Cochrane review injection of nonsteroidal anti-inflammatory drugs offered little or no benefit as compared with steroids [36].
Conservative treatment outcome for pediatric trigger thumb is somewhat controversial [37]. A study by Baek et al [38] on the natural history of pediatric thumb demonstrated that after a follow-up period of 5 years or more in patients who received no treatment for pediatric trigger thumb, complete resolution of flexion deformity occurred in 66 out of 87 thumbs (75.9%), and partial improvement occurred in the remaining 21 thumbs [25].
In another study, Lee et al [39], showed that extension splinting for 12 weeks led to improvement in 71% of thumbs, compared with 23% improvement in those patients who did not receive any treatment.
Surgical release
The chief indications for surgical management of TF are as follows:
Failure of splinting and/or injection treatment
Irreducibly locked TF
Trigger thumb in infants - Without surgical release, these infants are likely to develop a fixed flexion deformity of the interphalangeal (IP) joint
Although the results of percutaneous release are well established, the open technique is absolutely essential for the thumb or little finger or in the presence of proximal interphalangeal (PIP) contractures. Percutaneous release should be reserved for the index, middle, and ring fingers. [6, 7, 8, 9]
In a study from Oxford comparing percutaneous and open surgical methods, the two approaches displayed similar effectiveness, and both proved superior to conservative corticosteroid-injection treatment with regard to trigger cure and relapse rates [40].
In children, triggering has varying causes. Release of the A1 pulley alone does not always correct the problem. Additional treatment (eg, resection of one or both limbs of the flexor digitorum superficialis [FDS] tendon, A3 pulley release) may be required and is recommended in RA tenosynovitis. [9, 41, 42, 43].
In infants, the nodule on the flexor pollicis longus (FPL) tendon can be resected with good results. Corticosteroid injections are generally not helpful in these cases of trigger thumb.
Complications of Surgery
Complications of surgery include the following:
Radial digital nerve injury- There is a risk of radial nerve injury during surgery for trigger thumb due to its superficial location and oblique orientation. A digital nerve and artery repair may be necessary.
Bowstringing- Bowstringing may occur due to damage to the A2 or A4 pulley. Pulley reconstruction may be required.
Scar tenderness
Stiffness
Tendon scoring (percutaneous technique)
Wound dehiscence
Prognosis
Progressive symptoms begin with pain over the A1 pulley and progress to a fixed flexed digit. The prognosis is favorable in non-diabetic patients.
Relief with injections alone is achieved in up to 90% of non-diabetics and relief with surgery is achieved in >90% of all patients
References
AAOS. Trigger finger. AAOS Essentials of Musculoskeletal Care. 6th ed. Burlington, MA: Jones & Bartlett Learning; 2022.
Finnoff JT, Johnson W. Upper limb pain and dysfunction. Cifu DX, Eapen BC, Johns JS, Kowalske KJ, Lew HL, Miller MA, et al, eds. Braddom's Physical Medicine and Rehabilitation. 6th ed. Philadelphia: Elsevier; 2021. 715-26.
Fam AG. Regional pain problems. Klippel JH, Dieppe PA, eds. Practical Rheumatology. London, England: Mosby; 1997.
Schubert C, Hui-Chou HG, See AP, Deune EG. Corticosteroid injection therapy for trigger finger or thumb: a retrospective review of 577 digits. Hand (N Y). 2013 Dec. 8 (4):439-44.
Rodgers WB, Waters PM. Incidence of trigger digits in newborns. J Hand Surg Am. 1994 May. 19 (3):364-8.
De Smet L, Steenwerckx A, Van Ransbeeck H. The so-called congenital trigger digit: further experience. Acta Orthop Belg. 1998 Sep. 64 (3):306-8.
Li Z, Wiesler ER, Smith BP, Koman LA. Surgical treatment of pediatric trigger thumb with metacarpophalangeal hyperextension laxity. Hand (N Y). 2009 Dec. 4 (4):380-4.
Marks MR, Gunther SF. Efficacy of cortisone injection in treatment of trigger fingers and thumbs. J Hand Surg Am. 1989 Jul. 14 (4):722-7.
Breen TF. Wrist and hand. Steinberg GG, Akins CM, Baran DT, eds. Orthopaedics in Primary Care. 3rd ed. Baltimore: Lippincott Williams & Wilkins; 1999. 99-138.
Brinker MR, Miller MD. The adult hand. Fundamentals of Orthopaedics. Philadelphia: WB Saunders; 1999. 196-220.
Magee DJ, Manske RC. Forearm, wrist, and hand. Orthopedic Physical Assessment. 7th ed. St Louis: Elsevier; 2022. 482-577.
Miyamoto H, Miura T, Isayama H, Masuzaki R, Koike K, Ohe T. Stiffness of the first annular pulley in normal and trigger fingers. J Hand Surg Am. 2011 Sep. 36 (9):1486-91.
Hueston JT, Wilson WF. The aetiology of trigger finger explained on the basis of intratendinous architecture. Hand. 1972 Oct. 4 (3):257-60.
Sampson SP, Badalamente MA, Hurst LC, Seidman J. Pathobiology of the human A1 pulley in trigger finger. J Hand Surg Am. 1991 Jul. 16 (4):714-21.
Ryzewicz M, Wolf JM. Trigger digits: principles, management, and complications. J Hand Surg Am. 2006 Jan. 31 (1):135-46.
Kumar P, Chakrabarti I. Idiopathic carpal tunnel syndrome and trigger finger: is there an association?. J Hand Surg Eur Vol. 2009 Feb. 34 (1):58-9.
Grandizio LC, Beck JD, Rutter MR, Graham J, Klena JC. The incidence of trigger digit after carpal tunnel release in diabetic and nondiabetic patients. J Hand Surg Am. 2014 Feb. 39 (2):280-5.
Freiberg A, Mulholland RS, Levine R. Nonoperative treatment of trigger fingers and thumbs. J Hand Surg Am. 1989 May. 14 (3):553-8.
Griggs SM, Weiss AP, Lane LB, Schwenker C, Akelman E, Sachar K. Treatment of trigger finger in patients with diabetes mellitus. J Hand Surg Am. 1995 Sep. 20 (5):787-9.
Stahl S, Kanter Y, Karnielli E. Outcome of trigger finger treatment in diabetes. J Diabetes Complications. 1997 Sep-Oct. 11 (5):287-90.
Baumgarten KM, Gerlach D, Boyer MI. Corticosteroid injection in diabetic patients with trigger finger. A prospective, randomized, controlled double-blinded study. J Bone Joint Surg Am. 2007 Dec. 89 (12):2604-11.
Moriya K, Uchiyama T, Kawaji Y. Comparison of the surgical outcomes for trigger finger and trigger thumb: preliminary results. Hand Surg. 2005 Jul. 10 (1):83-6.
Masquijo JJ, Ferreyra A, Lanfranchi L, Torres-Gomez A, Allende V. Percutaneous trigger thumb release in children: neither effective nor safe. J Pediatr Orthop. 2014 Jul-Aug. 34 (5):534-6.
Leung OY, Ip FK, Wong TC, Wan SH. Trigger thumbs in children: results of surgical release. Hong Kong Med J. 2011 Oct. 17 (5):372-5.
Baek GH, Lee HJ. The natural history of pediatric trigger thumb: a study with a minimum of five years follow-up. Clin Orthop Surg. 2011 Jun. 3 (2):157-9.
Moore JS. Flexor tendon entrapment of the digits (trigger finger and trigger thumb). J Occup Environ Med. 2000 May. 42 (5):526-45.
Bae DS. Pediatric trigger thumb. J Hand Surg Am. 2008 Sep. 33 (7):1189-91.
Kim HR, Lee SH. Ultrasonographic assessment of clinically diagnosed trigger fingers. Rheumatol Int. 2010 Sep. 30 (11):1455-8.
Drossos K, Remmelink M, Nagy N, de Maertelaer V, Pasteels JL, Schuind F. Correlations between clinical presentations of adult trigger digits and histologic aspects of the A1 pulley. J Hand Surg Am. 2009 Oct. 34 (8):1429-35.
Tung WL, Kuo LC, Lai KY, Jou IM, Sun YN, Su FC. Quantitative evidence of kinematics and functional differences in different graded trigger fingers. Clin Biomech (Bristol, Avon). 2010 Jul. 25 (6):535-40.
Lapidus PW, Guidotti FP. Stenosing tenovaginitis of the wrist and fingers. Clin Orthop Relat Res. 1972 Mar-Apr. 83:87-90.
Rhoades CE, Gelberman RH, Manjarris JF. Stenosing tenosynovitis of the fingers and thumb. Results of a prospective trial of steroid injection and splinting. Clin Orthop Relat Res. 1984 Nov. 236-8.
de Boer P, Buckley R, Hoppenfeld S. The wrist and hand. Surgical Exposures in Orthopaedics: The Anatomic Approach. 6th ed. Philadelphia: Wolters Kluwer; 2022. 197-276.
[Guideline] Huisstede BM, Hoogvliet P, Coert JH, Fridén J, European HANDGUIDE Group. Multidisciplinary consensus guideline for managing trigger finger: results from the European HANDGUIDE Study. Phys Ther. 2014 Oct. 94 (10):1421-33.
Murphy D, Failla JM, Koniuch MP. Steroid versus placebo injection for trigger finger. J Hand Surg Am. 1995 Jul. 20 (4):628-31.
Leow MQH, Zheng Q, Shi L, Tay SC, Chan ES. Non-steroidal anti-inflammatory drugs (NSAIDs) for trigger finger. Cochrane Database Syst Rev. 2021 Apr 14. 4:CD012789.
Patel MR, Bassini L. Trigger fingers and thumb: when to splint, inject, or operate. J Hand Surg Am. 1992 Jan. 17 (1):110-3.
Baek GH, Kim JH, Chung MS, Kang SB, Lee YH, Gong HS. The natural history of pediatric trigger thumb. J Bone Joint Surg Am. 2008 May. 90 (5):980-5.
Lee ZL, Chang CH, Yang WY, Hung SS, Shih CH. Extension splint for trigger thumb in children. J Pediatr Orthop. 2006 Nov-Dec. 26 (6):785-7.
Sato ES, Gomes Dos Santos JB, Belloti JC, Albertoni WM, Faloppa F. Treatment of trigger finger: randomized clinical trial comparing the methods of corticosteroid injection, percutaneous release and open surgery. Rheumatology (Oxford). 2012 Jan. 51 (1):93-9.
Cardon LJ, Ezaki M, Carter PR. Trigger finger in children. J Hand Surg Am. 1999 Nov. 24 (6):1156-61.
Ashford JS, Bidic SM. Evaluation of pediatric trigger thumb in the Hispanic population at a southwest urban medical center. Plast Reconstr Surg. 2009 Oct. 124 (4):1221-1224.
Herren DB, Chung KC. Rheumatoid arthritis and other inflammatory arthropathies. Wolfe SW, Pederson WC, Kozin SH, Cohen MS, eds. Green's Operative Hand Surgery. 8th ed. Philadelphia: Elsevier; 2022. Vol 2: 2040-104.