Peripheral Nerve Injury & Repair
Dr. KS Dhillon
Introduction
Insights of neuronal injury and repair date back to early periods. It dates back specifically to Galen in the second century AD [1]. The research on this topic has been increasing continuously and several nerve repair techniques have developed over time. It has been estimated that about 2–3% of all patients admitted to Level I trauma centers suffer from peripheral nerve injuries [2]. Cervical spine injury occurs in up to 3–6% of all patients with trauma [3]. This means that CNS injuries are almost doubled when compared to the peripheral nerve injuries. Although peripheral nerve repair is not a life-saving surgery, it has been proven to be a life-changing surgery, with significant benefits to the patient’s quality of life. Since most patients with peripheral nerve injuries are from the working-age population, peripheral nerve repair also has substantial socioeconomic implications [4].
Peripheral nerves provide the path for all types of axons that compose the peripheral nervous system such as the motor and sensory axons. Injuries to these nerves are common due to their scarce physical protection and superficial position throughout the human body.
Depending on the type and extent of injury, an extensive array of symptoms
and outcomes are possible. The symptoms will depend on the severity, type of trauma, age, and type of nerves involved [5].
Much awareness and information already exist on the natural mechanisms of nerve injury and regeneration. However, effective regenerative treatments that ensure complete functional and sensory recovery are rare [6,7].
To understand the phenomena of nerve injury and repair, the basic anatomy of peripheral nerves has to be known (Figure 1).
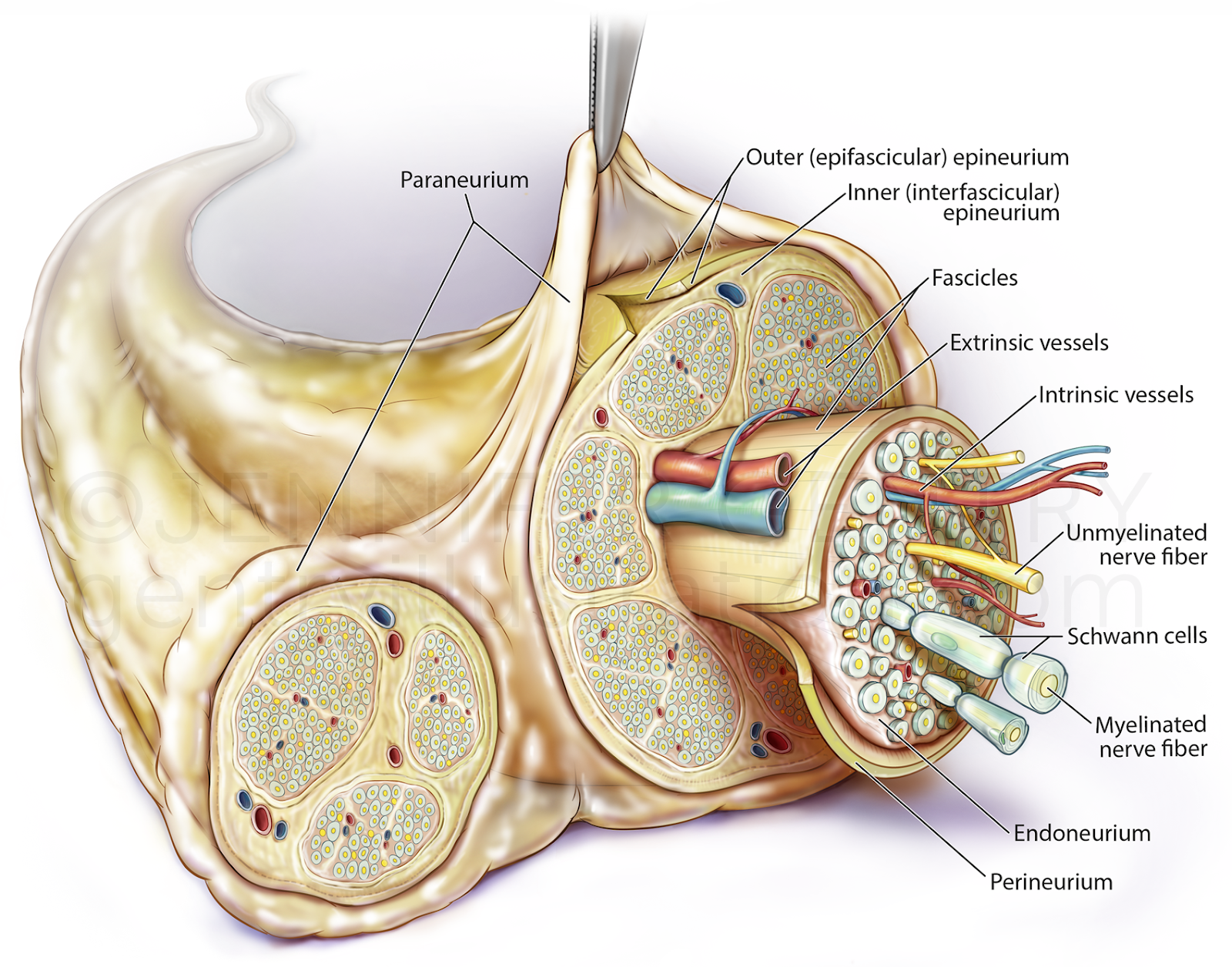
Fig 1 Nerve anatomy
A peripheral nerve is made up of multiple fascicles. Groups of fascicles are separated by the epineurium. Multiple axons form a fascicle. The fascicle is surrounded by a perineurium. The axons are surrounded by the endoneurium. External to the perineurium is the blood supply derived from major arteries.
After the injury, the process of Wallerian degeneration starts [8]. The
nerve stumps distal to the injury site will experience cellular variations despite the fact that the cells themselves were not injured. The axons start to collapse. The Schwann cells discard their ensheathing myelin and macrophages are recruited.
The macrophages remove degenerated axons, myelin debris, and Schwann cells [9]. After a few days, Schwann cells de-differentiate owing to their lost connection with axons, starting a vigorous proliferation. Galectin-3 plays a key role in activating myelin phagocytosis. Macrophages and Schwann
cells are promoted to degrade myelin, thus having major importance in the degeneration process [10].
The pre-existent and the recently produced Schwann cells, align together to form the bands of Bungner, which are highly aligned fibers formed by the basal lamina of the Schwan cells. These bands are responsible for guiding the axon and their growth cones, from the proximal to the distal site, across the gap. The growth cones can extend at a rate of 1–3 mm a day [11]. The Schwann cells affect peripheral nerve repair in three distinct manners. These include proliferation, development of bands of Bungner, and secretion of adequate growth factors [12].
After the nerve injury, the process of Wallerian degeneration starts immediately [13]. The nerve stumps distal to the injury site will experience cellular variations despite the fact that the cells themselves were not injured. The axons start to collapse, Schwann cells discard their ensheathing myelin and macrophages are recruited. After a few days, Schwann cells de-differentiate due to their lost connection with axons and start to vigorously proliferate. Galectin-3 plays a key role in activating myelin phagocytosis. The macrophages and Schwann cells are promoted to degrade myelin [14].
Presentation and Pathophysiology of Nerve Injuries
Peripheral nerve injuries in the upper extremity are very common. The patient is usually young and sustains a laceration from a sharp metal object or from a machine [15]. A detailed medical history is taken. The sensation is tested. Vibration is tested using a tuning fork. Two-point discrimination is tested by using a paper clip. This is good for testing group A axons slow fibers. The pick-up test is useful to test sensibility and tactile gnosis where the patient picks up the instructed item from a table full of multiple objects [16,17]. Sudomotor activity can be assessed in children by the absence of wrinkling after water immersion or in adults using the sweat test [17]. The motor function is tested and graded from 0-5.
Electromyography (EMG), nerve conduction studies, or electrical muscle stimulation tests can be used to confirm a nerve injury. Most commonly nerve conduction studies are used. The test assesses the number of remaining functional axons. These tests are useful in compressive lesions and partial lesions 5-7 days following the injury. Doppler studies are useful to assess the blood flow to the nerve. Ischaemia can cause direct damage to the motor and sensory nerves.
The sequel of nerve regeneration involves a series of regulated steps. Understanding this sequel of events is important for determining the timing and techniques of nerve repair [18].
During the first few hours following the nerve injury chromatolysis and swelling takes place in the cell body and the nucleus [18]. For the first few days oedema and swelling continues in the axonal stump. Within two to three days Wallerian degeneration commences. This involves axonal and myelin disintegration both in an antergrade and retrograde direction [18].
Schwann cells and macrophage infiltration occurs to remove cell debris, leaving the basement membrane for about 3-6 weeks [19]. Schwann cells start to proliferate, organize and guide the axonal sprouts between the basement membranes of the two nerve ends [18]. Nerve regeneration begins on the columns of Schwann cells and these are called Bunger bands. The intact proximal axon then sprouts a growth cone. The lamellipodia and filopodia cytoplasmic extensions allow the axon to explore the new environment and help in guiding the nerve repair. Actin found in the axon allows elongation inside the tube. Growth continues at the rate of 1-3 mm/day. The scar tissue interferes with the growth [18].
Classification of Nerve Injuries
Nerve injuries were classified by Seddon et al [20] into neuropraxia, axonotmesis, and neurotmesis. Sunderland expanded on this classification taking into consideration the histological diagnosis [21].
Neuropraxia (Sunderland Type 1)
This is an injury to the myelin sheath only and the axonal sheath is preserved. It is classified as the least severe nerve injury [20]. This injury usually results from compression or stretching. No Wallerian degeneration occurs. Recovery occurs within days or weeks [20].
Axonotmesis (Sunderland Type 2-4)
In this type of injury the axon is affected and Wallerian degeneration occurs distal to the site of injury [20]. In type 2 injuries only the axon is involved. In type 3 injury there is disruption of the endoneurium. In type 4 injury the perineurium is involved [20]. In type 2 injuries full recovery usually occurs. In types 3 and 4 injuries failure of full recovery can be expected. In type 4 injuries surgical intervention is required. Most surgeons advocate an 8-10 week wait to ensure that they do not improve spontaneously [20].
Neurotmesis (Sunderland Type 5) ‘Neuroma-in-Continuity’
This is the most severe type of injury. In this type of injury complete disruption of the nerve occurs with transection of the epineurium. Surgical intervention is required in such cases [20].
Timing of Nerve Repair
Primary repair for peripheral nerve injuries takes place within the first couple of days [22]. Secondary repair takes place a week or more after the injury [22]. Partial injuries, which constitute 15% of the nerve injuries, result from stretch or contusions of the nerve. They are usually managed with secondary repair [23-25]. For complete injuries, the method of repair will depend on what is found during the nerve exploration. If the epineurium is found to be neatly divided then primary repair without tension is usually undertaken. If the ends are ragged then a graft may be required [26].
Technique of Nerve Repair
The most commonly used nerve repair technique is a primary end-to-end repair. In the initial preparation stage, the nerve ends are prepared by removal of any necrotic tissue present. After removal of necrotic tissue two normal looking ends will be seen. The joint above the nerve injury is flexed to bring the two ends together. In some cases bone shortening may be necessary to bring the two ends together [27].
The nerve ends are mobilized and brought together. Tensionless repairs have better outcomes. During the approximation of the nerve ends extensive intrafasicular dissection has to be avoided [27]. The blood vessels must be aligned and proper rotational alignment must be maintained [27].
The nerve is repaired by suturing the epineurium with 9-0 or 10-0 non-absorbable sutures. Sometimes individual fascicular groups are identified for repair. These types of repair are usually used to repair larger nerves where sensory and motor fibers can be repaired separately [28].
Postoperatively nerve repairs are protected by immobilization for 10-14 days. Sometimes surgeons advocate up to six weeks of immobilization depending on the nerve injury severity [27]. After this period passive and active range of motion is initiated [27]. Age is the most vital factor to determine the outcome of nerve repair [29].
End-to-side nerve repair can also be done. This involves the attachment of one or two distal injured nerve end to the side of the uninjured nerve. This technique is useful when the ends are not available as sources of axons [30].
Why is Regeneration Following Nerve Repair Incomplete?
The decision to operate is usually delayed several weeks following the nerve injury to see if spontaneous recovery occurs. During this wait atrophy of motoneurons occurs which is only partially reversible [31]. The velocity of growth is only 1-3 mm/day and so there is time for neurotrophic factor production in the distal segments of the nerve to fall preventing fast regeneration [32,33]. A major factor affecting nerve repair is that the axotomized nerve needs to cross the coaptation site, which occurs in a random manner and the axon may fail to reach the distal stump altogether [34]. Another factor that affects the gaining of adequate repair is the misalignment of the motor and sensory axons. If motor axons enter sensory end organs they are ‘pruned’ in a process called preferential motor reinnervation [35]. Alternatively, muscle axons towards muscle can result in random innervation of the wrong muscles [36]. Furthermore, after a long period of inactivity, the target muscles that the nerves are trying to reinnervate may have undergone denervation-induced atrophy, producing adverse clinical outcomes [32].
Other Techniques For Nerve Repair
Nerve Grafting
In patients with severe nerve injuries, the defect between the two nerve ends can be too large for end-to-end repair. In such patients, the defect has to be bridged by using a nerve graft [37,38].
Usually nerve grafts are autologous sensory nerves. These include the medial or lateral antebrachial cutaneous nerves, dorsal cutaneous nerve branch of the ulnar nerve, lateral femoral cutaneous nerve, and superficial sensory branch of the radial nerve [37,38]. The length of the nerve gap to be repaired, donor site morbidity, and dissection difficulty has to be taken into account when considering the most appropriate nerve to use [37,38]. To achieve full recovery nerves should be grafted within six months. The graft harvested is usually 10-20% longer than the measured defect to allow for contraction [37,38]. Postoperative splinting is usually done for 1-14 weeks, to achieve satisfactory clinical outcome. Nerve harvesting can be associated morbidity at the donor site. Only about 40-50% of patients with nerve grafts achieve notable functional improvement [39].
Improving Autologous Nerve Grafts
A study by Boyd and Gordon [40] showed that long-term continuous treatment with exogenous glial cell line-derived neurotrophic factor (GDNF) significantly increased the number of motoneurons that regenerate their axons, completely reversing the negative effects of chronic axotomy.
Application of electrical stimulation to peripheral nerves improves peripheral nerve lesions gaps. It shortens the delay of fibers crossing the nerve injury site and not the speed of fiber growth. The effects of electrical stimulation is only short lasting. There is no difference in effect after three months [41,42]. Phototherapy that uses low-power laser therapy has also been tried [43]. It improves axon regeneration and myelination. There are, however, limited reports to support the use of laser therapy [43].
Replacing Autologous Nerve Grafts
Autologous biological tissues/non-nerve grafts have been considered as an alternative as these non-nerve grafts would be immunologically compatible and non-toxic. However, harvesting these samples with appropriate size and dimensions is usually difficult. Autogenous vein grafts have been used as conduits for nerve regeneration [44]. Skeletal muscle tissue has also been used as graft material for nerve repair [45].
Non-autologous sources can be used to bridge the gap between nerve lesions. These tissues offer an unlimited supply. They, however, have an associated immunogenic risk, including the transmission of disease and graft versus host disease reactions.
Considerations For Replacements of Autologous Nerve Grafts
When constructing a nerve conduit for nerve repair there are four elements that need to be taken into consideration. The first element is the scaffold for axonal proliferation, then the support cells for Schwann cells, and lastly the growth factors and extracellular matrix.
Scaffolds
The scaffold is a structure for supporting axonal regeneration [46]. Natural materials have been tested. These include laminin, fibronectin, and collagen due to their advantages of decreased toxic effect, improved biocompatibility, and enhancement of the migration of support cells [46]. However, there is documented evidence that they lose their ability to regenerate when stored for long periods of time [47].
Synthetic materials have been used and tested as scaffolds. They are useful since they can be manipulated to the exact configuration needed. The long-term consequences of the conduit on the nerve remains unknown.
Supports Cells, Growth Factors, and the Extracellular Matrix
Support cells (SCs) increase axon migration and produce structural and adhesive extracellular matrix (ECM) molecules that promote nerve regeneration. Investigators have used SC for CNS and PNS regeneration [48,49,50]. There are numerous growth factors that are involved with peripheral nerve repair. These include nerve growth factor (BGF), brain derived neurotrophic factor (BDNF), platelet-derived growth factors (PDGF), fibroblast growth factor (FGF), insulin-like growth factor (IGF-1, IGF-2), and ciliary neurotrophic factor (CNTF). These growth factors can be directly incorporated into the nerve conduit [51,52,53].
The ECM molecules are important for axonal extension. They guide the nerve regeneration. The ECM molecules including fibronectin, collagen, and laminin are incorporated into the conduit. They act as a guidance channel [54,55].
Nerve Transfers
The use of nerve transfers is becoming more frequent. In this procedure less needed nerve fascicles from a donor nerve are transected, dissected, and then attached to a more important distal nerve segment. The procedure transforms a proximal nerve injury into a distal one with short regeneration [56]. This technique is often used for transferring nerve trunks in patients with brachial plexus injury.
Examples of nerve transfers include the transfer of the thoracodorsal nerve to the deltoid muscle for axillary nerve lesions and the pronator quadratus branch of the anterior interosseous never transfer to the motor branch of the ulnar nerve at the Guyon’s canal [56].
Gene Therapy
Gene therapy offers another alternative to autologous nerve grafts for peripheral nerve repair. The main advantages of gene therapy are that the transduced cells will express the gene for an extended period of time which is useful since the neurotrophic factors inserted usually have a short half life [57]. The expression in the selected cells is restricted to the cell at the site of the injection of the viral vector. Hence, the therapy is selective, localized, and specific.
Several vectors are being investigated and tested with different types of neurotrophic factors but the main three cellular targets for gene therapy are the Schwann cells, injured neurons, and the muscle fibers. So far gene therapy has been successfully tested in rodent models to counteract the atrophy of spinal motor neurons following ventral root avulsion [58].
Selective viral over expression of nerve growth factor in the sensory saphenous branch results in increased correct sensory reinnervation after injury. This could help the challenge of misrouting the regenerating sensory axons [59]. Studies have shown that the long-term expression of neurotrophic factors by Schwann cells in the injured nerve is possible with gene therapy [60,61].
Conclusion
The clinical outcome after nerve repair is often inadequate. Hence over the last decade, there has been extensive research into alternatives for surgical repair [62-65]. The concept of using a nerve conduit for peripheral nerve repair is quicker and avoids harvesting morbidity but it has not resulted in better outcomes so far. Many growth factors have been identified that influence nerve regeneration. This provides hope for the development of the ideal combination of growth factor and nerve conduit. Many conduits are currently being studied but they are still in their experimental stage. Few have been approved for clinical application.
References
Nawabi, D. H., Jayakumar, P., and Carlstedt, T. (2006). Peripheral nerve surgery. Ann. R. Coll. Surg. Engl. 2006, 88, 327–328. doi: 10.1308/rcsann.
Noble, J., Munro, C. A., Prasad, V. S. S. V., and Midha, R. Analysis of upper and lower extremity peripheral nerve injuries in a population of patients with multiple injuries. J. Trauma Acute Care Surg. 1998, 45, 116–122.
Ghafoor, A. U., Martin, T. W., Gopalakrishnan, S., and Viswamitra, S. Caring for the patients with cervical spine injuries: what have we learned? J. Clin. Anesth. 2005, 17, 640–649.
Wojtkiewicz, D. M., Saunders, J., Domeshek, L., Novak, C. B., Kaskutas, V., and Mackinnon, S. E. Social impact of peripheral nerve injuries. Hand. 2015, 10, 161–167.
Siemionow, M., and Brzezicki, G. “Chapter 8: Current techniques and concepts in peripheral nerve repair,” in International Review of Neurobiology (Academic Press), 2009, 141–172.
Grinsell, D., and Keating, C. P. Peripheral nerve reconstruction after injury: a review of clinical and experimental therapies. Biomed Res. Int. 2014:698256.
He, B., Zhu, Z., Zhu, Q., Zhou, X., Zheng, C., Li, P., et al. Factors predicting sensory and motor recovery after the repair of upper limb peripheral nerve injuries. Neural Regen. Res.2014. 9, 661–672.
Rotshenker, S. (2011). Wallerian degeneration: the innate-immune response to traumatic nerve injury. J. Neuroinflammation 8:109.
Deumens, R., Bozkurt, A., Meek, M. F., Marcus, M. A., Joosten, E. A., Weis, J., et al. Repairing injured peripheral nerves: bridging the gap. Prog. Neurobiol. 2010, 92, 245–276.
Pesheva, P., Nellen, J., Biersack, H.-J., and Probstmeier, R. Galectin-3 is differentially expressed during peripheral nerve development: dependence on the Schwann cell phenotype. Neurosci. Res. Commun. 2002, 30, 71–82.
Griffin, J. W., Hogan, M. V., Chhabra, A. B., and Deal, D. N. Peripheral nerve repair and reconstruction. J. Bone Joint Surg. Am. 2013, 95, 2144–2151.
Jessen, K. R., Mirsky, R., and Lloyd, A. C. Schwann cells: development and role in nerve repair. Cold Spring Harb. Perspect. Biol. 2015, 7:a020487.
Rotshenker, S. Wallerian degeneration: the innate-immune response to traumatic nerve injury. J. Neuroinflammation. 2011, 8:109.
Pesheva, P., Nellen, J., Biersack, H.-J., and Probstmeier, R. Galectin-3 is differentially expressed during peripheral nerve development: dependence on the Schwann cell phenotype. Neurosci. Res. Commun. 2002, 30, 71–82.
McAllister RM, Gilbert SA, Calder JS, Smith PJ. The epidemiology and management of upper limb peripheral nerve injuries in modern practice. J Hand Surg. 1996;21B:4–13.
Omer GE. Methods of assessment of injury and recovery of peripheral nerves. Surg Clin North Am. 1981;61:303.
O’Riain S. New and simple test of nerve function in hand. Br Med J. 1973;3:615–6.
Deumens R, Bozkurt A, Meek MF , et al. Repairing injured peripheral nerves: Bridging the gap. Prog Neurobiol. 2010;92(3): 245–76.
Fu SY, Gordon T. The cellular and molecular basis of peripheral nerve regeneration. Mol Neurobiol. 1997;14:67–116.
Seedon HJ, editor. London:: Her Majesty’s Stationery Office; 1954. Peripheral nerve injuries Medical Research Council Special Report Series 282.
Sunderland S. Rate of regeneration of I: sensory nerve fibers and II: motor fibers. Arch Neurol Psychiatry. 1947;58:1–14.
Slutsky DJ, Hentz VR, Jabaley M, editors. Philadelphia:: Churchill Livingstone Elsevier.; 2006. Primary nerve repair Peripheral nerve surgery: Practical applications in the upper extremity. pp. 23–38.
Kline DG. Physiological and clinical factors contributing to the timing of nerve repair. Clin Neurosurg. 1977;24:425–55.
Kline DG, Hackett ER. Reappraisal of timing for exploration of civilian peripheral nerve injuries. Surgery. 1975;78(1):54–65.
Brown PW. Factors influencing the success of the surgical repair of peripheral nerves. Surg Clin North Am. 1972;52:1137–55.
Seddon HJ, editor. 2nd ed. Edinburgh:: Churchill Livingstone; 1972. Surgical Disorders of the Peripheral Nerves.
Mackinnon SE, Dellon AL, editors. New York:: Theime Medical Publishers; 1988. Surgery of the peripheral Nerve.
Young L, Wray RC, Weeks PM. A randomized prospective comparison of fascicular and epineural digital nerve repairs. Plast Reconstr Surg. 1981;68:89–93.
RosÉn B, Lundborg G, Dahlin LB, Holmberg J, Karlsson B. Nerve repair: Correlation of restitution of functional sensibility with specific cognitive capacities. J Hand Surg. 1994;19b:452–8.
Bontioti E, Kanje M, Lundborg G, Dahlin LB. End-to-side nerve repair in the upper extremity of rat. J Peripher Nerv Syst. 2005; 10:58–68.
Fu SY, Gordon T. Contributing factors to poor functional recovery after delayed nerve repair: Prolonged denervation. J Neurosci. 1995;15:3886–95.
Eggers R, Tannemaat MR, Ehlert EM, Verhaagen J. A spatio-temporal analysis of motoneuron survival, axonal regeneration and neurotrophic factor expression after lumbar ventral root avulsion and implantation. Exp Neurol. 2010;223:207–20.
Hoke A, Redett R, Hameed H , et al. Schwann cells express motor and sensory phenotypes that regulate axon regeneration. J Neurosci. 2006;26:9646–55.
McDonald D, Cheng C, Chen Y, Zochodne D. Early events of peripheral nerve regeneration. Neuron Glia Biol. 2006;2:139–47.
Madison RD, Archibald SJ, Lacin R, Krarup C. Factors contributing to preferential motor reinnervation in the primate peripheral nervous system. J Neurosci. 1999;19:11007–16.
Ijkema-Paassen J, Meek MF, Gramsbergen A. Reinnervation of muscles after transection of the sciatic nerve in adult rats. Muscle Nerve. 2002;25:891–7.
Terzis JK, Millesi H. Nerve grafting Clinic in Plastic Surgery Philadelphia. WB Saunders. 1984:105–13.
Gerlberman RH, Millesi H, editors. Operative Nerve Repair and Reconstruction Vol 1. Philadelphia:: JB Lipincott.; 1991. Indications and techniques of nerve grafting. pp. 525–43.
Lee SK, Wolfe SW. Peripheral nerve injury and repair. J Am Acad Orthop Surg. 2000;8:243–52.
Boyd JG, Gordon T. Glial cell line-derived neurotrophic factor and brainderived neurotrophic factor sustain the axonal regeneration of chronically axotomized motoneurons in vivo. Exp Neurol. 2003; 183:610–9.
Ahlborn P, Schachner M, Irintchev A. One hour electrical stimulation accelerates functional recovery after femoral nerve repair. Exp Neurol. 2007;208:137–44.
Irintchev A, Angelov DN, Guntinas-Lichius O. Regeneration des, N. facialis im Vergleich zu anderen peripheren Nerven (German). Hals-Nasen-Ohren Heilkunde (HNO). 2010;58:426–32.
Van Breugel HH, Bar PR. He-Ne laser irradiation affects proliferation of cultured rat Schwann cells in a dose-dependent manner. J Neurocytol. 1993;22:185–90.
Chiu DTW. Autogenous vein graft as a conduit for nerve regeneration. Surgery. 1982;91:226–32.
Meek MF, Varejao AS, Geuna S. Use of skeletal muscle tissue in peripheral nerve repair: review of the literature. Tissue Eng. 2000; 10:1027–36.
Wang KK, Costas PD, Bryan DJ, Jones DS, Seckel BR. Insideout vein graft promotes improved nerve regeneration in rats. J Reconstruc Microsurg. 1993;14:608–18.
Gulati AK. Peripheral nerve regeneration through short- and long-term degenerated nerve transplants. Brain Res. 1996;742:265–70.
Woerly S, Plant GW, Harvey AR. Neural tissue engineering: From polymer to biohybrid organs. Biomaterials. 1996;17:301–10.
Zhang Y, Campbell G, Anderson PN, Martini R, Schachner M, Lieberman AR. Molecular basis of interactions between regenerating adult rat thalamic axons and Schwann cells in peripheral nerve grafts II: Tenascin-c. J Comp Neurol. 1995;361:210–24.
Zhang Y, Campbell G, Anderson PN, Martini R, Schachner M, Lieberman AR. Molecular basis of interactions between regenerating adult rat thalamic axons and schwann cells in peripheral nerve grafts I: Neural cell adhesion molecules. J Comp Neurol. 1995; 361:193–209.
Griffin CC, Letourneau PC. Rapid retraction of neurites by sensory neurons in response to increased concentrations of nerve growth factor. J Cell Biol. 1980;86:156–61.
Yip HK, Rich KM, Lampe PA, Johnson EM JR. The effects of nerve growth factor and its antiserum on the postnatal development and survival after injury of sensory neurons in the rat dorsal root ganglia. J Neurosci. 1984;4:2986–92.
Sterne GD, Brown RA, Green CJ, Terenghi G. Neurotrophin-3 delivered locally via fibronectin mats enhances peripheral nerve regeneration. Eur J Neurosci. 1997;9:1388–96.
Valentini RF, Aebischer P, Winn SR, Galletti PM. Collagen and laminin containing gels impede peripheral nerve regeneration through semipermeable nerve guidance channels. Exp Neurol. 1987;98:350–35.
Williams LR, Danielsen N, Muller H, Varon S. Exogenous matrix precursors promote functional nerve regeneration across a 15-mm gap within a silicone chamber in the rat. J Comp Neurol. 1987; 264:284–90.
Nath RK, Mackinnon SE. Nerve transfers in the upper extremity. Hand Clin. 2000;16:131–9.
Hoyng SA, Tannemaat MR, De Winter F, Verhaagen J, Malessy MJA. Nerve surgery and gene therapy: a neurobiological and clinical perspective. J Hand Surg Eur Vol. 2011;36:735.
Eggers R, Tannemaat MR, Ehlert EM, Verhaagen J. A spatio-temporal analysis of motoneuron survival, axonal regeneration and neurotrophic factor expression after lumbar ventral root avulsion and implantation. Exp Neurol. 2010;223:207–20.
Hu X, Cai J, Yang J, Smith GM. Sensory axon targeting is increased by NGF gene therapy within the lesioned adult femoral nerve. Exp Neurol. 2010;223:153–65.
Haastert K, Grothe C. Gene therapy in peripheral nerve reconstruction approaches. Curr Gene Ther. 2007;7:221–8.
Tannemaat MR, Verhaagen J, Malessy M. The application of viral vectors to enhance regeneration after peripheral nerve repair. Neurol Res. 2008;30:1039–46.
Chimutengwende-Gordon M, Khan WS. Recent advances and developments in neural repair and regeneration for hand surgery. Open Orthop J. 2012;6(1):103–7.
Rayanmarakkar F, Khan WS, Hardingham TE. In: Hand Surgery: Preoperative Expectations, Techniques and Results. In: Beckingsorth RH., editor. Principles of Tissue Engineering Approaches for Tendons, Skin, Nerves and Blood Vessels in the Hand. New York: Nova Science Publishers.; 2009. pp. 85–96.
Picardo NE, Khan WS. Tissue engineering applications and stem cell approaches to the skin, nerves and blood vessels. Curr Stem Cell Res Ther. 2012;7(2):115–21.
Khan WS, Pastides P, Khan WS, Pastides P, Hardingham TE, editors. New York: : Nova Science Publishers.; 2012. Tissue Engineering Approaches for Neurovascular Structure Tissue Engineering and the Musculoskeletal System: A Limitless Cure. pp. 107–18.
No comments:
Post a Comment