Olecranon fractures
Dr K Dhillon
Introduction
Ten percent of fractures around the elbow are olecranon fractures [1]. There is a diverse array of treatment options that have continued to evolve for the management of this fracture. These fractures vary in their complexity from relatively straightforward transverse fractures to comminuted and unstable configurations. No particular mode of treatment can be universally applied to the diverse array of fracture patterns encountered. For appropriate management of these fractures, the surgeon needs to have a good understanding of the anatomy, treatment options available, and potential complications.
Anatomy
The elbow is a complex hinge joint with a flexion arc of 0–150 degrees (fig1). The joint is stabilized by a number of factors. These include the anterior coronoid process and the posterior olecranon process which resist the translational forces of the humerus on the ulna.
The ulna collateral ligament and the radial head provide resistance to valgus stress. The lateral collateral ligament complex counters the varus stress.
Hyaline cartilage lines the articular surfaces. A transverse bare area devoid of cartilage is found at the midpoint between the coronoid and the tip of the olecranon [2]. The trochlea notch of the ulna, which articulates with the trochlea of the humerus has a transverse ‘‘bare area’’ at the junction between the anterior third and the posterior two-thirds.
This area varies in size between individuals. In one cadaveric study of 39 elbows, the mean width was 5.3 mm [3]. Knowledge of this area is important when reducing olecranon fractures. It can be tempting, but not correct, to eliminate any articular surface that is not covered by cartilage.
The triceps muscle inserts into the posterior third of the olecranon and the proximal ulna. It blends with the aponeurosis overlying the anconeus and the common extensor mechanism. The brachialis inserts into the coronoid process of the ulna and along with the triceps helps to produce compressive forces across the elbow joint during contraction.
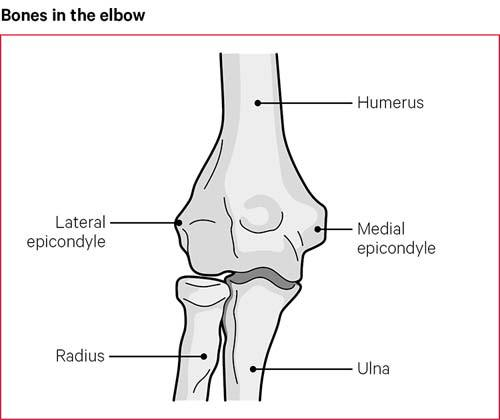
Fig 1.
Patella cubiti, an accessory ossicle embedded in the distal triceps may be present and can sometimes be mistaken for a fracture [4].
The ulnar nerve passes around the posterior aspect of the medial epicondyle and between the two heads of the flexor carpi ulnaris. The flexor carpi ulnaris spans in an arcade-like manner from the medial epicondyle to the olecranon process to form the roof of the cubital tunnel. The nerve lies posterior to the ulnar collateral ligament, which forms the floor of the cubital tunnel. The ulna collateral ligament attaches in a fanlike fashion to the medial border of the olecranon. The brachialis tendon inserts onto the proximal ulnar metaphysis distal to the tip of the midportion of the anterior coronoid.
Mechanism of injury
Direct or indirect trauma can cause fractures of the olecranon. A fall or blunt trauma on the posterior aspect of the elbow can cause a fracture directly. Indirect trauma from forces generated within the triceps muscle can occur with eccentric contraction during a fall on a partially flexed elbow leading to a fracture of the olecranon. Amis and Miller [5], in a cadaveric model, investigated the effect of impact mechanisms on olecranon fracture patterns. They found that the radial head and coronoid fractures occurred from impact to the forearm with the elbow in 80 degrees of flexion or less. Olecranon fractures followed direct blows at 90 of flexion. Distal humerus fractures were caused by impact when the elbow was in greater than 110 degrees of flexion. In cases of severe force to the elbow, a fracture dislocation can occur with posterior displacement of the olecranon fragment and the distal ulnar fragment together with the head of the radius.
Classification
There are multiple classification systems for olecranon fractures. None have, however, gained widespread acceptance. Colton et al [6] were the first, to develop a system based on the displacement and character of the fracture:
Type I fractures are undisplaced fractures
Type II fractures are unstable fractures. They are subdivided according to fracture pattern: type IIA avulsion fractures, type IIB transverse or oblique fractures, type IIC isolated comminuted fractures and type IID are fracture-dislocations.
The AO classification of proximal radius and ulna fractures are divided into three broad groups. Type A are extra-articular fractures of either radius or ulna. Type B are intraarticular fractures of either bone, with type B1 being specifically an intra-articular fracture of the olecranon alone, and type C fractures are intra-articular fractures of both radius and ulna [7].
The Schatzker classification is based on the fracture pattern and a
consideration of the type of internal fixation that is required [8]. In type A the fracture line is transverse. In type B the fracture line is also transverse but there is impaction of bone. In type C the fracture line is oblique. In type D there is a comminuted fracture. In type E the fracture line is oblique and distal to the articular surface. In type F there is a fracture dislocation.
The Mayo Clinic classification is one of the most frequently used and describes fractures on the basis of stability, displacement, and comminution:
Type I- the fractures are undisplaced and stable
Type II- the fractures are displaced and unstable with intact collateral ligaments preventing dislocation
Type III- the fracture is with an unstable elbow joint
Type II and III fractures are further subdivided into A where the fracture is non-comminuted and B where the fracture is comminuted [9]. The Schatzker and Mayo classifications can be useful in predicting prognosis. Schatzker types C (oblique) and D (comminuted) and Mayo type III fractures are associated with less favorable outcomes [10].
Diagnosis
History
Patients who have olecranon fractures and associated injuries present with pain and swelling around the elbow and distal arm. Patients with displaced fractures have an obvious deformity, and attempted motion can elicit painful crepitus. The patient is asked how the injury occurred. The patient is also asked about any associated neurovascular complications. A history of any concurrent illnesses precipitating the injury is obtained. A detailed account of comorbid conditions is important.
Clinical examination
An assessment of the soft tissues around the elbow is carried out during physical examination. There is usually extensive swelling with ecchymosis. The presence of abrasions or lacerations should be noted. There should be no aggressive assessment of range of motion or strength of the elbow.
A palpable sulcus may be present at the site of the olecranon fracture. There will be painful limitation of the range of motion of the elbow. There will be an inability to extend the elbow actively against gravity. A careful neurovascular examination is carried out before any planned manipulation of the elbow.
Radiographic and imaging assessment
Plain radiographs usually provide sufficient information for an accurate diagnosis. Severe comminution with displacement and overlap of bone fragments can obscure the fracture pattern. Radiographs have to be of good quality, out of splint and obtained while maintaining gentle longitudinal traction with the inclusion of the elbow joint on the film. Poor X-rays done in a splint are not as well suited for accurate diagnosis, classifying the fracture, and formal preoperative planning. Radiographs are carefully evaluated for the presence of associated injuries, such as a radial head fracture or dislocation, a distal humerus fracture, or a coronoid fracture. A CT scan rarely provides additional information that helps in decision making, and preoperative planning with an isolated olecranon fracture. It should be reserved for more complex fractures.
Treatment
Nondisplaced fractures of the olecranon (Mayo type IA and IB) are treated conservatively. Nondisplaced fractures are those where the displacement is less than 2 mm and there is no change in position with gentle flexion to 90 or extension of the elbow against gravity. These fractures are treated with a
long arm cast with the elbow in 90 of flexion for 3 to 4 weeks. After the cast is removed protected range of motion exercises are started. Flexion past 90 degrees is avoided until bone healing is complete at approximately 6 to 8 weeks. In elderly patients, the range of motion exercises can be started earlier than 3 weeks if patients can tolerate it so that stiffness can be prevented. After application of the cast, a follow-up radiograph should be done within 5 to 7 days to ensure that displacement of the fracture has not occurred. Immobilization in full extension is not done because stiffness is more likely. Fractures that require full extension for reduction should be treated surgically.
Tension band wire
Displaced olecranon fractures require surgical treatment to restore joint
congruity, elbow extension, and elbow stability. Transverse fractures without comminution (Mayo type IIA) can be treated by tension band wiring. A tension band wire construct converts the tensile distraction force of the triceps into a dynamic compressive force across the olecranon articular surface. K-wires are used for tension band wiring. Intramedullary cancellous screw fixation cannot be used in elderly patients who have osteoporosis.
Two 1.6-mm or 2.0-mm K-wires are inserted into the olecranon tip and the wires engage distally in the anterior cortex of the ulna [11]. Overpenetration of the wires should be avoided to prevent neurovascular damage, limitation of forearm rotation, or heterotopic ossification. Once the wire penetrates the far cortex, it is partially backed out and bent 180 degrees at the previously noted position and cut. The fibers of the triceps tendon are split sharply with a scalpel at the site of the K-wires to allow the cut and bent ends to be impacted against the cortex. A figure-of-8 loop of 18-gauge or 1.5-mm gauge wire is passed through a drill hole located distally. The hole is drilled approximately and equal distance from the fracture as the tip of the olecranon. The wire is then passed deep to the fibers of the triceps, near the bone, beneath the K-wires. The wire is then tightened by twisting in two places on opposite arms of the crossed portion of the figure-of-8.
The K-wires are seated firmly in the bone using an impactor, beneath the fibers of the triceps.
In transverse fractures with comminution (Mayo type IIB), the tension band technique cannot be used. It will collapse the fragments together, leading to a narrowed olecranon articulation that does not track properly. These fractures are treated with limited-contract dynamic compression (LCDC) plate fixation, with or without bone graft [12]. Similarly, a plate with lag screw fixation is preferred for oblique fractures or unstable displaced olecranon fracture–dislocations with and without comminution (Mayo type IIIA and IIIB).
Limited-contract dynamic compression plate fixation
LCDC plate fixation has several advantages [13,14]. The plate allows improved contouring. It can be appropriately placed on the dorsal tension surface of the proximal ulna around the tip of the olecranon. It helps to hold the proximal fragment when poor bone quality limits screw purchase. The redesigned screw holes allow greater angulation of screw placement and the option of compression from either side of the screw hole. Furthermore, its lower profile allows its use in subcutaneous situations where soft tissue coverage is minimal. Fixation of the plate proximally is often the greatest challenge because the bone there can be thin, and cancellous screws rather than cortical screws are used in elderly patients. The newer precontoured plates allow for an increased number of fixation points in the proximal fragment. In complex fractures of the proximal ulna, a large coronoid fragment is usually present. This fragment is very important to the final stability of the elbow. It must be fixed with lag screws placed either through or adjacent to the implanted plate [15]. Mobilizing the proximal olecranon fragment allows the coronoid to be visualized and reduced through the olecranon fracture.
Technique
The patient is placed in a lateral position on the operating table with the injured arm on a bolster across the chest. A tourniquet is placed on the upper arm. Skin preparation and draping is carried out. A posterior midline incision centered on the olecranon is made and extended proximally 5 cm from the tip of the olecranon. The ulna is exposed along its subcutaneous border. The anconeus can be elevated to approach the radial head if required. Impacted articular fragments are elevated. The coronoid is then reduced and provisionally fixed to the ulna with K-wires. A narrow 3.5-mm LCDC plate is then contoured to fit the proximal ulna. The plate is bent near 90, between the second and third screw holes of the plate. After the fracture is reduced the contoured plate is applied to the dorsal aspect of the olecranon. The plate is fixed proximally with one screw obliquely upward into the coronoid process. Fixation of the coronoid can also be performed with lag screws adjacent to the plate. Additional screws are placed proximally in the olecranon. The plate is secured distally to the shaft with three or four bicortical screws.
In patients with osteoporotic olecranon, direct trauma to the posterior aspect of the elbow can lead to severely comminuted fractures. In such situations, excision of the fracture fragments and reattachment of the triceps tendon may be necessary in elderly patients whose olecranon fracture fragments are too small or too comminuted for internal fixation.
The coronoid and anterior soft tissues, collateral ligaments, and interosseus membrane must be intact. The triceps tendon is reattached adjacent to the articular surface with nonabsorbable sutures that are passed through drill holes in the proximal ulna. Reattaching the triceps this way creates a sling for the trochlea. There is a smooth congruent transition from the triceps tendon to the articular surface but it decreases the moment arm. This can result in a weaker extensor mechanism but elbow stability is enhanced [16]. The amount of olecranon that can be safely excised remains debatable. Based on in vitro [17] and clinical studies [18,19] between 50% and 70% of the olecranon articular surface can be excised without compromising elbow stability as long as the coronoid and distal trochlea are preserved.
Complications
Painful hardware irritation is one of the most common complication after
internal fixation of olecranon fractures. Such a complication has been reported in up to 80% of cases. The incidence of prominent painful hardware is more after tension band wiring as compared to compression plating [20,21]. Simpson and colleagues [13] reported no cases of symptomatic hardware irritation after LCDC plating. Bailey and colleagues [22], however, reported that 20% of their patients required plate removal because of the prominence of the plate fixation.
Loss of movements is usually not a significant problem in patients with isolated olecranon fractures. In patients with isolated olecranon fractures, the typical loss of motion is 10 to 15 degrees of extension. Patients who have associated fractures of the radial head or coronoid are more likely to develop limitations of motion.
Nonunion of olecranon fractures has been reported in up to 1% of the patients. The typical symptoms of nonunion are pain, instability, or loss of motion [23]. Treatment options for olecranon nonunions
include:
Excision of the olecranon fragment.
Osteosynthesis with a LCDC plate, and bone grafting.
Elbow arthroplasty in the presence of severe posttraumatic arthritis.
In elderly patients, acceptable management includes excision of the proximal portion of the pseudarthrosis and repair of the triceps tendon, making sure that the coronoid and anterior soft tissues are intact.
Rehabilitation
Early initiation of physical therapy is one of the most important issues in
elbow surgery especially in the elderly. Postoperatively, a posterior POP slab with the elbow flexed to 90 degrees is applied to help manage postoperative pain. The posterior slab is usually discontinued after 5 to 7 days and a removable splint is provided to the patient. Gentle active assisted exercises and passive motion exercises are then started. The patient is told to support the wrist with the opposite hand and gently flex and extend the elbow. The arm is taken out of the splint several times a day for these exercises and to let gravity work on extending the elbow. Active motion against resistance is avoided until callus formation is evident. This usually happens at 8 to 10 weeks. If the stability of the fixation is in doubt, then a hinged fracture brace can be used to provide additional support.
Results and outcome
The clinical outcomes after fractures of the olecranon are generally good to excellent. Most series report satisfactory outcomes and restoration of normal or near-normal function in more than 95% of patients.
Bailey et al [22] evaluated the functional outcome of plate fixation for displaced olecranon fractures (Mayo type II or III) in 25 patients at an average follow-up of 34 months. They found that the patient satisfaction was high (9.7/10) with a low pain rating (1/10). Based on the Mayo elbow score, 22 patients had excellent or good outcomes. The mean DASH score showed almost normal upper extremity function.
Karlsson et al [24] evaluated the long-term outcome of closed olecranon fractures in 73 patients at a mean of 19 years after the fracture. The primary treatment consisted of open reduction and internal fixation in 84% of the elbows. Of these patients, 61 had no complaints at follow-up, 9 had occasional pain, and 3 had daily pain. Ninety-six percent of the patients had an excellent or good overall outcome.
Conclusion
About 10% of the fractures around the elbow are olecranon fractures. There is a diverse array of treatment options that have continued to evolve for the management of this fracture. Some of these fractures are relatively straightforward transverse fractures and others are comminuted and unstable. No particular mode of treatment can be universally applied to the diverse array of fracture patterns encountered. For appropriate management of these fractures, the surgeon needs to have a good understanding of the anatomy, treatment options available, and potential complications.
Olecranon fractures have good to excellent outcomes with adherence to a treatment algorithm based on displacement, comminution, and joint stability. Decreased range of motion, radiographic evidence of degenerative changes, and requirement for hardware removal are common. These can be minimized through careful attention to proper technique, anatomic reduction with stable fixation, and early mobilization.
References
Rommens PM, Kuchle R, Schneider RU, Reuter MM. Olecranon fractures in adults: factors influencing outcome. Injury 2004; 35:1149–57.
Stormont TJ, An KN, Morrey BF, et al. Elbow joint contact study: comparison of techniques. J Biomech 1985;18(5):329–36.
Wang A, Mara M, Hutchinson DT. The proximal ulna: an anatomic study with relevance to olecranon osteotomy and fracture fixation. J Shoulder Elbow Surg 2003;12(3):293–6.
Winter M, Balaguer T, Tabutin J. Bilateral patella cubiti. A case report. J Bone Joint Surg Am 2006; 88(2):415–7.
Amis AA, Miller JH. The mechanisms of elbow fractures: an investigation using impact tests in vitro. Injury 1995;26(3):163–8.
Colton CL. Fractures of the olecranon in adults: classification and management. Injury 1973;5(2):121–9.
Lavigne G, Baratz M. Fractures of the olecranon. J Am Soc Surg Hand 2004;4(2):94–102.
Browner BD, Jupiter JB, Levine AM, et al. Skeletal trauma. Philadelphia: Saunders; 1992.
Morrey BF. Current concepts in the treatment of fractures of the radial head, the olecranon, and the coronoid. J Bone Joint Surg Am 1995; 77:316–27.
Rommens PM, Kuchle R, Schneider RU, Reuter MM. Olecranon fractures in adults: factors influencing outcome. Injury 2004; 35:1149–57.
Prayson MJ, Williams JL, Marshall MP, et al. Biomechanical comparison of fixation methods in transverse olecranon fractures: a cadaveric study. J Orthop Trauma 1997;11(8):565–72.
Hak DJ, Golladay GJ. Olecranon fractures: treatment options. J Am Acad Orthop Surg 2000;8(4): 266–75.
Simpson NS, Goodman LA, Jupiter JB. Contoured LCDC plating of the proximal ulna. Injury 1996; 27(6):411–7.
McKee MD, Seiler JG, Jupiter JB. The application of the limited contact dynamic compression plate in the upper extremity: an analysis of 114 consecutive cases. Injury 1995;26(10):661–6.
Doornberg J, Ring D, Jupiter JB. Effective treatment of fracture-dislocations of the olecranon requires a stable trochlear notch. Clin Orthop Relat Res 2004;429:292–300.
Coonrad RW, Morrey BF. Management of olecranon fractures and nonunion. In: Morrey BF, editor. Master techniques in orthopaedic surgery: the elbow. 2nd edition. Philadelphia: Lippincott Williams & Wilkins; 2002. p. 103–26.
An KN, Morrey BF, Chao EY. The effect of partial removal of proximal ulna on elbow constraint. Clin Orthop Relat Res 1986;209:270–9.
Inhofe PD, Howard TC. The treatment of olecranon fractures by excision or fragments and repair of the extensor mechanism: historical review and report of 12 fractures. Orthopedics 1993;16(12): 1313–7.
Gartsman GM, Sculco TP, Otis JC. Operative treatment of olecranon fractures. Excision or open reduction with internal fixation. J Bone Joint Surg Am 1981;63(5):718–21.
Hume MC, Wiss DA. Olecranon fractures. A clinical and radiographic comparison of tension band wiring and plate fixation. Clin Orthop Relat Res 1992;285:229–35.
Wolfgang G, Burke F, Bush D, et al. Surgical treatment of displaced olecranon fractures by tension band wiring technique. Clin Orthop Relat Res 1987;224:192–204.
Bailey CS, MacDermid J, Patterson SD, et al. Outcome of plate fixation of olecranon fractures. J Orthop Trauma 2001;15(8):542–8.
Papagelopoulos PJ, Morrey BF. Treatment of nonunion of olecranon fractures. J Bone Joint Surg Br 1994;76(4):627–35.
Karlsson MK, Hasserius R, Karlsson C, et al. Fractures of the olecranon: a 15- to 25-year followup of 73 patients. Clin Orthop Relat Res 2002;403:205–12.
No comments:
Post a Comment