Bunionette Deformity (Tailor's Bunion)
Dr. KS Dhillon
Introduction
Bunionette refers to a prominence on the lateral aspect of the fifth metatarsal head. It may or may not be symptomatic. Bunionettes have traditionally been referred to as “tailor’s bunion” since it is prevalent among tailors, who sit cross-legged all day with the lateral edge of their feet rubbing on the ground. There are specific risk factors that predispose patients to this deformity. The deformity is usually treated conservatively. Surgical intervention may be needed for patients who continue to experience pain and disability.
Anatomy and pathophysiology
Symptomatic bunionette deformities are often associated with anatomic variations. Coughlin in 1990 (1) described several anatomic factors that can contribute to symptomatic bunionette deformities. These include:
Congenital plantarflexed or dorsiflexed metatarsals
Increased four to five intermetatarsal angle (IMA)
Prominence of the metatarsal head
Lateral bowing of the metatarsal shaft
Typically the toe is adducted at the MP joint (fig 1). Congenital deformities such as brachymetatarsia and splayfoot have been linked to the development of bunionette deformities (2,3). Soft tissue abnormalities can accompany bunionette deformities. Ankle and hindfoot deformities and plantarflexed metatarsals are associated with plantar callosity and increased pressure on wearing shoes (4).

Fig 1.
Evaluation
The bunionette deformity is more common in women than men. The reported ratios vary from 2:1 to 10:1. Bilateral deformity is common (5). Patients with symptomatic bunionette deformities usually present with pain at the lateral side of the forefoot. The pain is usually exacerbated by wearing closed shoes. Some patients have more pain in the plantar-lateral forefoot rather than on the lateral side. Other metatarsophalangeal (MTP) joint pathologies have to be ruled out during the examination. Non-Inflammatory, crystal, and inflammatory arthropathies have to be ruled out. In patients with suspected inflammatory arthritis, the rheumatoid nodules should be evaluated with ultrasound or MRI to assess the extent of the disease. The deformity and prominence in such cases are caused by chronic synovitis. The chronic synovitis causes capsular distension (6). Sometimes chronically inflamed bursal tissue can develop lateral to the bony prominence. This can worsen the clinical picture.
A complete ankle and foot examination is necessary to define the exact pathology and also to identify other co-existing pathologies. The clinician should look for pes planus and hindfoot (1,7,8). Splayfoot deformity arises When there are coexisting hallux valgus and bunionette deformities, splayfoot deformity arises (2). Coughlin carried out a study in 20 patients (30 feet) with symptomatic bunionettes refractory to conservative treatment who underwent longitudinal diaphyseal osteotomy, lateral condylectomy, and distal metatarsophalangeal realignment and found that 60% of patients required correction of additional deformities including hallux valgus, hallux rigidus, and hammertoe deformities, among others (30%, 10% and 7%, respectively (9). Examination of the skin and subcutaneous tissue is important. Lateral eminence swelling with either keratosis, erythema, ulceration, or callosity has to be evaluated. Callosity can be present on the plantar aspect or laterally. In patients where these lesions extend to the plantar surface, elevation of the metatarsal head in addition to medialization should be carried out (4,10).
Radiographic examination starts with standard weight-bearing X-rays with anterior posterior and lateral views. There are several angles that have been described in the assessment of bunionette deformity. Most often, the 5th MTP joint angle (MTP-5 angle), the 4–5 IMA, and the fifth metatarsal lateral deviation angle are measured. The average MTP-5 angle is 10.2. Ninety percent of normal feet have an angle of 14 degrees or less (11).
The MTP-5 angle shows the medial deviation of the toe in relation to the metatarsal shaft. The average angle in normal feet is 10.2 degrees. In 90% of normal feet, the angle is 14 degrees or less (5,11). On average an MTP-5 angle of 16 degrees or more produces symptoms (4,5,9). Another angle that is commonly measured is the 4–5 IMA. The 4-5 IMA measures the divergence of the 4th and 5th metatarsals. When a line is drawn through the axis of each metatarsal, the 4–5 IMA angle is the angle at the intersection of the lines Fig 2.
The most common method to bisect The axis of the metatarsal can be bisected by using a line on the medial and lateral margins of the proximal metaphysis and the metatarsal neck (4,5,12). The average of the 4–5 IMA angle is 10.8 degrees (5). Fallat and Buckholz were of the opinion that the most consistent way to determine the axis of the 5th metatarsal shaft is to use a line adjacent and parallel to the medial surface of the proximal half of the metatarsal shaft (13).
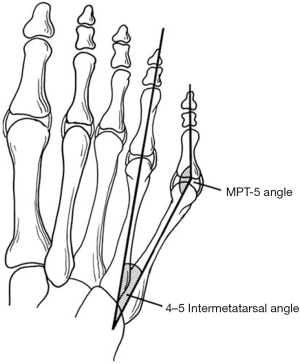
Fig 2.
When comparing normal feet (6.5 degrees) to feet with bunionettes (8.7 degrees) they found a difference of 2 degrees. They found a change in 4–5 IMAs when foot position goes from inversion to eversion. There was a change of 3 degrees in 4–5 IMAs (13). The consensus settled on abnormal 4–5 IMAs values equal to or greater than 9 (4).
Excessive lateral bowing of the fifth metatarsal shaft can contribute
to the development of a painful bunionette (1,4,9,14,15). In these patients, the 4–5 IMA may be normal. A lateral curvature of the 5th metatarsal diaphysis causes the deformity. According to Fallat and Buckholz, this measurement is the angle created by a line parallel and adjacent to the proximal medial surface of the fifth metatarsal and a line representing the axis of the distal metatarsal (13). Nestor et al (5) did not find a difference in lateral bowing between symptomatic bunionettes and controls. Fallat and Buckholz, however, found an average lateral bowing of 8.1 degrees compared to controls (2.6 degrees) (13). The estimated incidence of patients who undergo surgery for symptomatic bunionettes who present with bowing of the 5th metatarsal shaft ranges from 10% to 23% (4). The width of the 5th metatarsal head also contributes to symptomatic bunionettes. The normal width of the 5th metatarsal head is about 13 mm, and it varies from 11 to 14 mm (13,16). The incidence of an abnormally large metatarsal width ranges from 16% to 33% (4).
Classification
Coughlin suggested a classification system based on radiographic parameters for bunionettes that is widely used today (9).
Type 1 refers to an enlarged 5th metatarsal head
Type 2 refers to normal 4–5 IMA with an increased lateral bow of the 5th metatarsal shaft
Type 3 refers to an increased 4–5 IMA
Type 3 is the most common type in patients with symptomatic bunionettes. This makes the 4–5 IMA the most important factor to play a role in symptomatic bunionettes (4).
Nonoperative Treatment
Literature regarding successful nonsurgical treatment options for symptomatic bunionettes is limited. According to Shi et al more than 90% of patients with symptomatic bunionette deformities resolve without invasive treatment (7). Non-operative treatment should always be attempted before any surgery is carried out. Non-operative management usually involves symptomatic treatment of pain and the callosities. Shoe modification with a wider toe box can help patients control pain. Callosities can be managed with protective pads and shaving. Grice et al showed the efficacy of corticosteroid injections in the treatment of little toe MP joint synovitis (17). No long-term studies have, however, shown improvement of symptoms with non-surgical management.
Operative Treatment
The operative treatment of bunionette deformities will largely depend on the type of deformity. The classification system of bunionette deformities helps doctors establish an algorithm that can be used to treat these deformities. The surgical treatment options include:
Metatarsal head resection
Proximal or midshaft oblique osteotomies
Distal chevron osteotomies
Subcapital oblique osteotomies
Scarf osteotomy,
Ludloff variant osteotomy
Metatarsal head resection is associated with poor outcomes. It is only reserved for unhealthy patients, or in patients with an infectious or inflammatory process.
Kitaoka and Holiday reported poor results at 8 years follow-up in 7 patients (11 feet) undergoing metatarsal head resections (18). The poor outcomes included persistent lateral forefoot prominence, transfer metatarsalgia, and painful fifth toe deformity. The authors recommend against the use of metatarsal head resections. Nonetheless, metatarsal head resection does have a role in rheumatoid arthritis patients. In a retrospective study of 56 rheumatic feet, Reize et al showed successful results in terms of cosmetic and functional outcomes as well as pain control following resection of the first through fifth metatarsal heads for long-standing rheumatoid forefoot deformity (19).
Distal chevron osteotomy is a popular technique for the treatment of Type I bunionette deformities. Kitaoka et al performed 19 distal chevron metatarsal osteotomy operations in 13 patients with painful bunionettes. At a 7.1-year follow-up, they reported good outcomes without failures (20). The MTP 5 angle, IMA 4–5 angle, and forefoot width improved at follow-up. They had one case of transfer metatarsalgia and one case of wound infection. Boyer and Deorio reported good outcomes in 10 patients with symptomatic bunionette deformity who underwent 12 distal fifth metatarsal chevron osteotomies in which an absorbable poly-p-dioxanone suture (PDS) pin was used for fixation. All patients had radiographic union and high patient satisfaction (21).
Type I bunionette deformities can also be treated by a subcapital oblique osteotomy. Cooper and Coughlin in a retrospective review of 16 feet in 14 patients with a follow-up of approximately 3 years, showed good clinical results for correction of type I deformities (14). There was improved patient satisfaction and pain control. However, there was no significant improvement in IMA 4–5 angle post-operatively. This procedure has more flexibility than the chevron osteotomy. Besides translating the metatarsal head laterally, the metatarsal head can be elevated to alleviate plantar pressure.
Diaphyseal osteotomies are carried out when there is increased lateral bowing or IMA 4–5 angles. To correct bunionette deformities, Coughlin described an oblique osteotomy of the metatarsal shaft in conjunction with lateral condylectomy and distal MTP realignment. He reported 93% of good or excellent outcomes in 30 feet (9). More recently, Waizy et al showed improvement in patient satisfaction, lateral bowing, and radiographic measurements of IMA 4–5 angle with a reverse Ludloff osteotomy for type II and III bunionette deformities. They had no complications or revision procedures (22). Shi et al (7) reported several studies that reported similar outcomes with Ludloff variants and scarf osteotomies for type II and type III bunionette deformities.
Very proximal fifth metatarsal osteotomies are not recommended because of concerns of nonunion. Tenous blood supply to the proximal metaphyseal-diaphyseal region and higher stresses on the bone in this region can contribute to poor healing. Despite this, some doctors continue to carry out these osteotomies to address bunionette deformities with increased IMA 4–5 angles. Okuda et al (23) reported the outcome of proximal dome-shaped osteotomy in 8 patients (10 feet). They found significant improvement in MTP 5 angle and IMA 4–5 angles. The results were good in all 8 patients. There were, however, 3 cases of delayed union at the osteotomy site. They found that all 3 cases of delayed union had osteotomies that were more proximal than those with expected union rates. Therefore, they advised against performing osteotomies at sites that are too proximal.
In recent years, minimally invasive surgical techniques have become popular for several ankle and foot conditions. Giannini et al (24) reported excellent results in 32 patients (18 bilateral) using a transverse distal metatarsal osteotomy, for type II and III deformities. Waizy et al (25) reported their results using a similar technique in 31 feet. They, however, found good to excellent results in 16 feet, satisfactory in 14, and poor results in 9 feet. The results were inferior for type II and III deformities. According to them, this technique should only be used for type I deformity.
There are many variations in the post-operative care. Some doctors opt for non-weight bearing for 6 weeks. In these patients, the foot is placed in a splint following surgery and later a short leg cast is applied for 6 weeks. After 6 weeks the patient is allowed weight-bearing activities in a post-operative shoe. The patient is expected to return to normal activities at 8–10 weeks. Other doctors prefer a post-operative protocol that involves immediate heel-weight bearing in a post-operative shoe for 6 weeks. The patient is gradually allowed full weight bearing and is expected to return to normal activities between 8–10 weeks postoperatively.
Complications
The overall complication rate is low following correction of bunionette deformity (7). Some of the complications include:
Malunion
Nonunion
Recurrence
Wound complications
Avascular necrosis
Transfer metatarsalgia
Avascular necrosis and nonunion can result from excessive soft tissue stripping during the surgery. Inadequate immobilization of the osteotomy site due to poor or lack of internal fixation can also lead to nonunion and malunion. Extension of the proximal osteotomy into watershed areas can increase the risk of delayed union.
Since the metatarsal is small sized, distal osteotomies are at risk of instability due to poor fixation or overcorrection. Chevron osteotomies that translate more than 50% can lead to instability. Transfer metatarsalgia may occur if the fifth metatarsal is excessively elevated or shortened. The lateral dorsal cutaneous branch and sural nerve are at risk with any bunionette procedure and must be protected. A study by Malagelada et al (26) found that the nerve has variability and they described safe zones to protect it during minimally invasive techniques. When the procedure of choice fails to address the underlying driver of the deformity, recurrence of deformity is seen in all types of bunionette deformity. Hence, the chances of recurrence will be reduced if there is an adequate understanding of the types of deformities and the corresponding surgery.
Conclusions
Bunionette deformity is less common than hallux valgus and other forefoot disorders. It can, however, be a source of significant disability and pain. A proper evaluation is required with close examination of the entire ankle and foot. Initial treatment usually focuses on symptomatic relief. Several surgical options are available when conservative treatment fails. Excellent outcomes can be obtained with proper surgical selection and technique.
References
Coughlin MJ. Etiology and treatment of the bunionette deformity. Instr Course Lect 1990;39:37-48.
Bishop J, Kahn A, Turba JE. Surgical correction of the splayfoot: the Giannestras procedure. Clin Orthop Relat Res 1980;234-8.
Schimizzi A, Brage M. Brachymetatarsia. Foot Ankle Clin 2004;9:555-70.
Cooper MT. The Bunionette Deformity: Overview and Classification. Tech Foot Ankle Surg 2010;9:2-4.
Nestor BJ, Kitaoka HB, Ilstrup DM, et al. Radiologic anatomy of the painful bunionette. Foot Ankle 1990;11:6-11.
Brooks F, Hariharan K. The rheumatoid forefoot. Curr Rev Musculoskelet Med 2013;6:320-7.
Shi GG, Humayun A, Whalen JL, et al. Management of Bunionette Deformity. J Am Acad Orthop Surg 2018;26:e396-404.
Ceccarini P, Rinonapoli G, Nardi A, et al. Bunionette. Foot Ankle Spec 2017;10:157-61.
Coughlin MJ. Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Cooper MT, Coughlin MJ. Subcaptial Oblique Fifth Metatarsal Osteotomy Versus Distal Chevron Osteotomy for Correction of Bunionette Deformity. Foot Ankle Spec 2012;5:313-7.
Steel MW, Johnson KA, DeWitz MA, et al. Radiographic Measurements of the Normal Adult Foot. Foot Ankle 1980;1:151-8.
Schoenhaus H, Rotman S, Meshon AL. A review of normal inter-metatarsal angles. J Am Podiatry Assoc 1973;63:88-95.
Fallat LM, Buckholz J. An analysis of the tailor’s bunion by radiographic and anatomical display. J Am Podiatry Assoc 1980;70:597-603.
Cooper MT, Coughlin MJ. Subcapital oblique osteotomy for correction of bunionette deformity: medium-term results. Foot Ankle Int 2013;34:1376-80.
Yancey HA. Congenital lateral bowing of the fifth metatarsal. Report of 2 cases and operative treatment. Clin Orthop Relat Res 1969;203-5.
Zvijac JE, Janecki CJ, Freeling RM. Distal oblique osteotomy for tailor’s bunion. Foot Ankle 1991;12:171-5.
Grice J, Marsland D, Smith G, et al. Efficacy of Foot and Ankle Corticosteroid Injections. Foot Ankle Int 2017;38:8-13.
Kitaoka HB, Holiday AD. Metatarsal head resection for bunionette: long-term follow-up. Foot Ankle 1991;11:345-9.
Reize P, Leichtle CI, Leichtle UG, et al. Long-term results after metatarsal head resection in the treatment of rheumatoid arthritis. Foot ankle Int 2006;27:586-90.
Kitaoka HB, Holiday AD, Campbell DC. Distal Chevron metatarsal osteotomy for bunionette. Foot Ankle 1991;12:80-5.
Boyer ML, Deorio JK. Bunionette deformity correction with distal chevron osteotomy and single absorbable pin fixation. Foot ankle Int 2003;24:834-7.
Waizy H, Jastifer JR, Stukenborg-Colsman C, et al. The Reverse Ludloff Osteotomy for Bunionette Deformity. Foot Ankle Spec 2016;9:324-9.
Okuda R, Kinoshita M, Morikawa J, et al. Proximal dome-shaped osteotomy for symptomatic bunionette. Clin Orthop Relat Res 2002;173-8.
Giannini S, Faldini C, Vannini F, et al. The minimally invasive osteotomy “S.E.R.I.” (simple, effective, rapid, inexpensive) for correction of bunionette deformity. Foot ankle Int 2008;29:282-6.
Waizy H, Olender G, Mansouri F, et al. Minimally invasive osteotomy for symptomatic bunionette deformity is not advisable for severe deformities: a critical retrospective analysis of the results. Foot Ankle Spec 2012;5:91-6.
Malagelada F, Dalmau-Pastor M, Sahirad C, et al. Anatomical considerations for minimally invasive osteotomy of the fifth metatarsal for bunionette correction - A pilot study. Foot (Edinb) 2018;36:39-42.
No comments:
Post a Comment