Lateral Epicondylitis (Tennis Elbow)
Dr. KS Dhillon
Introduction
Lateral epicondylitis, also known as tennis elbow is an overuse injury secondary to an eccentric overload of the common extensor tendon at the origin of the extensor carpi radialis brevis (ECRB) tendon. Tennis elbow results from the repetitive strain caused by activities that involve repeated gripping and/or wrist extension. It is common in individuals who play squash, badminton, tennis, or any activity involving repetitive wrist extension, radial deviation, and/or forearm supination [1,2].
Etiology
Tennis elbow is an overuse injury. It is caused by repetitive strain from tasks and activities that involve loaded and repeated gripping and/or wrist extension. It is commonly seen in tennis players but can result from any sports that require repetitive wrist extension, radial deviation, and/or forearm supination. It is also seen in those who play squash and badminton, as well as other sports or activities that require similar movements. This condition is usually precipitated by poor mechanics and technique or improper equipment in athletic patients [3].
Anatomy
There is a common extensor origin on the lateral side of the elbow.
The extensor carpi radialis longus muscle originates from the lateral supracondylar ridge.
Muscles that originate on the lateral epicondyle include (Fig 1):
extensor carpi radialis brevis
extensor carpi ulnaris
extensor digitorum
extensor digiti minimi
anconeus
There is a lateral ulnar collateral ligament (LUCL) on the lateral side of the elbow.
The posterior interosseus nerve enters the supinator just distal to the radial head. Compression of the nerve can lead to radial tunnel syndrome. It may co-exist with lateral epicondylitis.
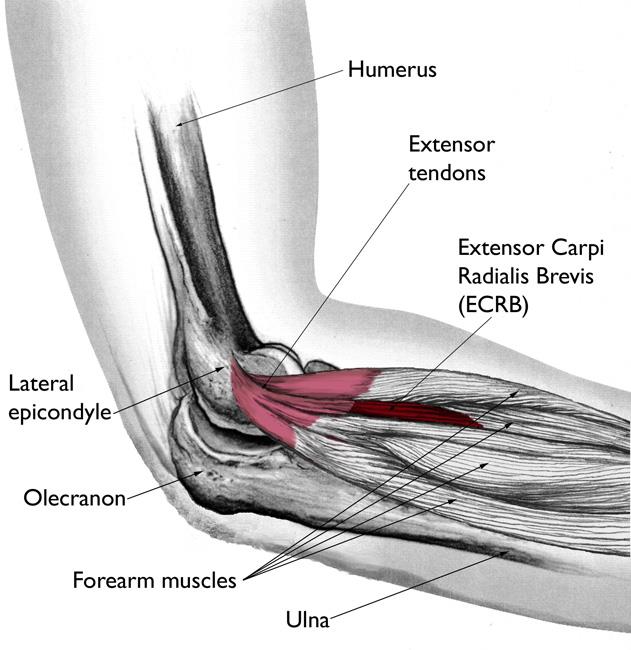
Fig 1.
Epidemiology
Tennis elbow is the most common cause of elbow pain. It tends to affect men and women equally. In the United States, the annual incidence is one to three percent. Although the condition is commonly referred to as tennis elbow, tennis players make up only 10% of the patient population. Half of the tennis players develop pain around the elbow. Of this, 75% have true tennis elbow.
Tennis elbow is more common in individuals who are older than 40 years. Obesity, smoking, repetitive movement for at least two hours daily, and vigorous activity such as managing physical loads over 20 kg are risk factors for developing this condition. The natural course of this condition is favorable. Spontaneous recovery occurs within one to two years in 80% to 90% of the patients [4,5,6].
Pathophysiology
Tennis elbow is primarily a degenerative overuse process of the common extensor tendon and the extensor carpi radialis brevis. Besides degenerative changes, the histological findings include granulation tissue, micro-rupture, an abundance of fibroblasts, unstructured collagen, vascular hyperplasia, and a notable lack of traditional inflammatory cells such as macrophages, lymphocytes, and neutrophils within the tissue. The term has previously been described as angiofibroblastic dysplasia based on multiple histologic studies [7,8]. Ultrasound examination often reveals calcifications, intra-substance tears, marked irregularity of the lateral epicondyle, as well as thickening and heterogeneity of the common extensor tendon [9].
Histopathology
Multiple studies reporting the histologic appearance of pathologic ECRB specimens show any combination of the following characteristics:[8]
Vascular hyperplasia
Hypertrophic or abundant fibroblasts
Collagen disorganization
Lack of inflammatory cells
History and Physical Examination
Patients usually report elbow pain of insidious onset. There will be an overuse history without a specific inciting traumatic event. The pain usually appears one to three days after an unaccustomed activity that involves repeated wrist extension.
There may be a history of new equipment use or an atypical workout such as an abnormally intense or prolonged workout. An acute injury or strain, such as lifting a heavy object or performing a hard backhand swing in tennis can also cause tennis elbow. This acute injury can lead to a more chronic process. The pain is usually over the lateral aspect of the elbow which worsens with activity and improves with rest. The pain can vary from being mild to severe. Mild pain can be seen with aggravating activities like tennis or the repeated use of a hand tool. Severe pain can be seen with simple activities like picking up and holding a coffee cup.
On examination, there is maximal tenderness over the lateral epicondyle. Occasionally the tenderness can be located distally about 1 cm to 2 cm from the lateral epicondyle. There may be some degree of tenderness and discomfort along the entire length of the tendon. The connecting muscle may exhibit tightness.
The patient’s pain increases and is reproduced with resisted wrist extension, especially when the elbow is extended and the forearm is pronated. Resisted extension of the middle finger when the elbow is extended is particularly painful due to increased stress placed on the tendon. There should be an absence of radicular symptoms such as numbness/tingling. These symptoms suggest radial nerve entrapment which can coexist [10].
Evaluation
Lateral epicondylitis is a clinical diagnosis. Imaging is not necessary. If other injury or condition is suspected then elbow radiographs can be obtained. Other conditions that would require radiographs would include concomitant degenerative joint disease, tumors, fractures, or bursitis. If the patient does not respond to nonoperative treatment then an MRI or ultrasound can be done to exclude tears, stress fractures, or osteochondral defects [11].
Management
Nonoperative Management
The first-line of treatment of lateral epicondylitis includes rest from offending activity as guided by the level of pain. Oral/topical NSAIDs and ice application after activity can be used to help with pain control. Forearm counterforce straps can be used to relieve tension at the lateral epicondyle. These are worn during activity. The role of counterforce straps is relatively controversial. A cock-up wrist splint can be used to take the stress off of the wrist extensors [10].
Occupational or physical therapy that focuses on forearm stretching and strengthening and progression to eccentric muscle strengthening of the common extensor tendon has also been found to be helpful. If the pain does not respond to such measures, more advanced or invasive techniques such as topical nitrates, botulinum toxin, autologous platelet-rich plasma, steroid injections, and dextrose prolotherapy can be utilized.
Surgical Management
Surgery is done as a last resort in the management of tennis elbow. Six to twelve months of nonoperative management should be attempted before considering surgical treatment. Surgery involves the release and debridement of extensor carpi radialis brevis (ECRB) origin.
During surgery, the incision is positioned over the common extensor origin. The ECRL is lifted off the ECRB which is located deep and posterior to ECRL. Degenerative tissue is excised. The epicondyle is decorticated. The capsule is repaired if it is breached. Side-to-side closure of the tendon is carried out. A generous debridement should be performed at the ECRB origin with confirmation of debridement of the pathologic tissue and stimulation of a healthy, bleeding, bony bed of tissue at the lateral epicondyle to help stimulate healing potential [12,13].
Differential Diagnosis
The differential diagnosis for lateral epicondylitis includes the following conditions:[14]
Elbow bursitis
Cervical radiculopathy
Posterolateral elbow plica
Posterolateral rotatory instability (PLRI)
Capitellar osteochondritis dissecans
Triceps tendinitis
Radiocapitellar osteoarthritis
Radial nerve entrapment
Radial tunnel syndrome
-palpation 3 to 4 cm distal and anterior to the lateral epicondyle
-pain with resisted middle finger extension
-pain with resisted forearm supination
Occult fracture(s)
Shingles
Prognosis
The prognosis for tennis elbow is generally good. Most patients get pain relief within 12 months of conservative treatment. For patients who do not improve with initial treatment with ice, rest, and NSAIDs, various physical and occupational therapies can be useful. Recurrence of symptoms will occur in patients who fail to follow through on their therapy plan.
Complications
Complications of lateral epicondylitis can include:
Recurrence of the injury when normal activity is resumed.
Rupture of the tendons with repeated steroid injections.
Failure to improve despite conservative treatment.
Postoperative complications can include the following:
Failing to address concomitant pathology
: Patients report inferior outcomes and lack of improvement if the
cause of symptoms is not addressed. The patients should be
educated regarding the risks and benefits of surgery. The former
include but are not limited to infection, blood loss, neurovascular
injury, continued pain, stiffness, or continued or worsening overall
dysfunction.
: Radial nerve entrapment can be missed or not addressed clinically in
up to 5% of patients being managed for lateral epicondylitis.
Iatrogenic LUCL injury
: Occurs iatrogenically with increased risk if the surgical dissection
extends beyond the radial head equator
: Postoperative iatrogenic posterolateral rotatory instability (PLRI) can
develop if the extension or LUCL compromise is significant.
Iatrogenic neurovascular injury
: Radial nerve injury
Heterotopic ossification
: Decrease risk via copious saline irrigation following decortication
and debridement
Infection
Patient Education
Patients need to receive counseling regarding prevention of strain and overuse to the forearm and elbow. Key counseling points can include:
Avoid end range of motion in both extension and flexion.
Use two hands to hold heavy tools, and use a two-handed backhand when playing tennis.
Limit repetitive grasping and gripping movements.
Avoid repetitive hand and wrist movements and take a break from such activities when necessary.
Avoid lifting heavy items with the arm in full extension and perform work or weight-lifting with the elbow partially bent.
If a movement causes the pain avoid it.
Conclusion
Tennis elbow is a very common condition and it affects men and women equally. It is an overuse injury primarily due to repetitive strain from tasks and activities that involve loaded and repeated gripping and/or wrist extension. It can occur from many types of sports including racquet sports, and golf. Most patients present with pain on the lateral side of the elbow. Patient education is an important part of the management. Individuals have to adopt good habits like stretching before taking part in intense physical activity. When there is pain it is important to rest the hand. Clinicians usually emphasize the importance of improving muscle strength and conditioning. Proper equipment or toolage use is important. With rest, most of the patients with tennis elbow improve within 3 to 18 months. Surgery is rarely required [15].
References
Welsh P. Tendon neuroplastic training for lateral elbow tendinopathy: 2 case reports. J Can Chiropr Assoc. 2018 Aug;62(2):98-104.
Kwapisz A, Prabhakar S, Compagnoni R, Sibilska A, Randelli P. Platelet-Rich Plasma for Elbow Pathologies: a Descriptive Review of Current Literature. Curr Rev Musculoskelet Med. 2018 Dec;11(4): 598-606.
Patiño JM, Corna AR, Michelini A, Abdon I, Ramos Vertiz AJ. Elbow Posterolateral Rotatory Instability due to Cubitus Varus and Overuse. Case Rep Orthop. 2018;2018:1491540.
Degen RM, Conti MS, Camp CL, Altchek DW, Dines JS, Werner BC. Epidemiology and Disease Burden of Lateral Epicondylitis in the USA: Analysis of 85,318 Patients. HSS J. 2018 Feb;14(1):9-14.
Chevinsky JD, Newman JM, Shah NV, Pancholi N, Holliman J, Sodhi N, Eldib A, Naziri Q, Zikria BA, Reilly JP, Barbash SE, Urban WP. Trends and Epidemiology of Tennis-Related Sprains/Strains in the United States, 2010 to 2016. Surg Technol Int. 2017 Dec 22;31:333-338.
Hassebrock JD, Patel KA, Makovicka JL, Chung AS, Tummala SV, Hydrick TC, Ginn JE, Hartigan DE, Chhabra A. Elbow Injuries in National Collegiate Athletic Association Athletes: A 5-Season Epidemiological Study. Orthop J Sports Med. 2019 Aug;7(8): 2325967119861959.
Kraushaar BS, Nirschl RP. Tendinosis of the elbow (tennis elbow). Clinical features and findings of histological, immunohistochemical, and electron microscopy studies. J Bone Joint Surg Am. 1999 Feb;81(2):259-78.
Nirschl RP, Pettrone FA. Tennis elbow. The surgical treatment of lateral epicondylitis. J Bone Joint Surg Am. 1979 Sep;61(6A):832-9.
Jeon JY, Lee MH, Jeon IH, Chung HW, Lee SH, Shin MJ. Lateral epicondylitis: Associations of MR imaging and clinical assessments with treatment options in patients receiving conservative and arthroscopic managements. Eur Radiol. 2018 Mar;28(3):972-981.
Ramage JL, Varacallo M. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Aug 30, 2022. Anatomy, Shoulder and Upper Limb, Wrist Extensor Muscles.
Nowotny J, El-Zayat B, Goronzy J, Biewener A, Bausenhart F, Greiner S, Kasten P. Prospective randomized controlled trial in the treatment of lateral epicondylitis with a new dynamic wrist orthosis. Eur J Med Res. 2018 Sep 15;23(1):43.
Sirico F, Ricca F, DI Meglio F, Nurzynska D, Castaldo C, Spera R, Montagnani S. Local corticosteroid versus autologous blood injections in lateral epicondylitis: meta-analysis of randomized controlled trials. Eur J Phys Rehabil Med. 2017 Jun;53(3):483-491.
Coombes BK, Bisset L, Vicenzino B. Management of Lateral Elbow Tendinopathy: One Size Does Not Fit All. J Orthop Sports Phys Ther. 2015 Nov;45(11):938-49.
Buchanan BK, Maini K, Varacallo M. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Sep 4, 2022. Radial Nerve Entrapment.
Nishizuka T, Iwatsuki K, Kurimoto S, Yamamoto M, Onishi T, Hirata H. Favorable Responsiveness of the Hand10 Questionnaire to Assess Treatment Outcomes for Lateral Epicondylitis. J Hand Surg Asian Pac Vol. 2018 Jun;23(2):205-209.
No comments:
Post a Comment