Quadrilateral Space Syndrome
Dr. KS Dhillon
Introduction
Quadrilateral space syndrome (QSS) is a rare disorder characterized by axillary nerve and posterior humeral circumflex artery (PHCA) compression within the quadrilateral space. It was first described by Cahill and Palmer in 1983 [1]. In the original description by Cahill, there were four distinct features of QSS. These included diffuse pain around the shoulder; paresthesia in a nondermatomal distribution; point tenderness above the quadrilateral space; and positive angiogram finding in provocative positioning [1]. The condition is usually attributed to repeated overhead activity such as seen in baseball and volleyball. However, a variety of other pathologies including hematomas, lipomas, and labral cysts may cause compression in the quadrilateral space [2].
Neurovascular compression accounts for the acute findings in QSS. These include pain, paraesthesia, and atrophy. It is uncertain whether this is primarily a problem of neural entrapment or vascular compression [3,4]. Compression may occur at rest or with movement. QSS should be considered in all patients with a complaint of shoulder pain, neck pain, lateral arm paraesthesia, and/or quadrilateral space tenderness [5].
Anatomy
The quadrilateral space lies between the teres minor muscle superiorly, the teres major muscle inferiorly, the long head of the triceps medially, and the humeral shaft laterally (Fig 1) [3]. The PHCA and axillary nerve reside in the quadrilateral space.
The axillary nerve innervates the teres minor and deltoid muscles. These two muscles are primarily responsible for abduction and external rotation. There are fibrous bands within the quadrilateral space, which exacerbate symptoms, particularly pain that is elicited by movements associated with the deltoid and teres minor muscles [6,7]. The anatomical differences in innervation patterns in the glenohumeral joint can make it difficult to distinguish whether the pain is due to suprascapular nerve palsy or axillary nerve compression [8]. Since the PHCA stretches around the neck of the humerus, repetitive tension and mechanical stress to the PHCA wall can lead to thrombosis and aneurysmal degeneration [9,10,11].
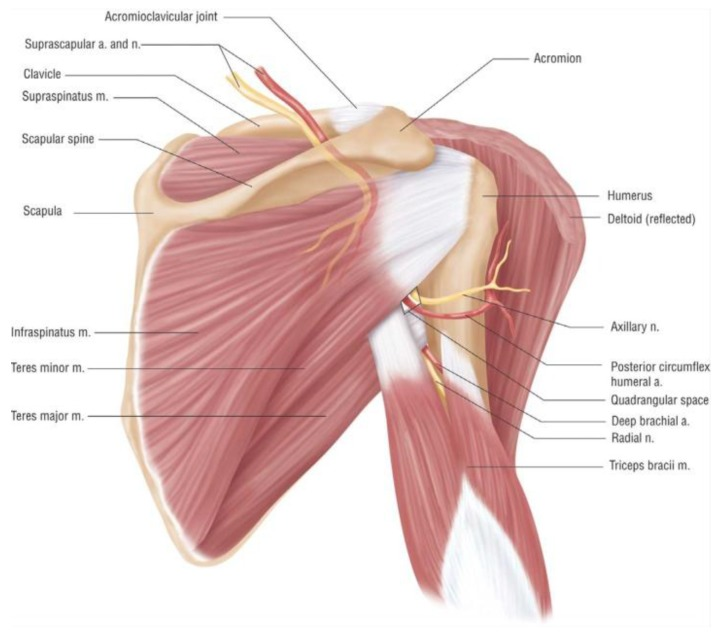
Fig 1.
Etiology
The etiology of QSS is not clear. Impingement is usually due to trauma, fibrous bands, or hypertrophy of a muscular border. Occasionally, QSS can also be caused by lipomas, labral cysts, hematoma resulting from fracture, osteochondroma, and axillary schwannomas. Compression of the axillary nerve can also be caused by aneurysms and traumatic pseudoaneurysms of the posterior circumflex humoral artery [11-14]. Anatomical variations can also predispose patients to QSS.
Abnormal origin of the radial collateral artery from the PHCA can also mimic the symptoms of QSS [15]. An accessory subscapularis muscle that originates from the anterior surface of the subscapularis, courses under the axillary nerve, and inserts onto the shoulder joint, can also serve as a risk factor for QSS [16]. QSS has also been seen as a rare complication of thoracic surgery [17].
Clinical Presentation
QSS is typically seen in younger patients who are less than forty years of age. Patients usually present with a history of repeated overhead activities as seen in athletes involved in volleyball, baseball, or swimming [18-25]. Symptoms can be vague. There can be neurogenic or vascular symptoms. Neurogenic symptoms include paresthesias, fasciculations, weakness, or neurogenic pain. Vascular symptoms include signs of acute ischemia such as pain, pallor, and absent pulses. Symptoms of thrombosis, or embolism such as coolness or cyanosis of the hand or digits may also be present. Besides vascular and neurogenic symptoms, patients with QSS can experience muscular atrophy and accompanying weakness. This is believed to be due to denervation. There can be tenderness over the quadrilateral space. In some severe cases, thrombosis of the PHCA can block flow from the axillary artery, leading to embolization and subsequent digital ischemia, cyanosis, and cold intolerance [9,26,27].
Differential Diagnoses
The symptoms of QSS are nondescript. This often makes QSS a diagnosis of exclusion since it can mimic other vascular, musculoskeletal, or nerve-related syndromes in the area. A review of the patient’s medical history can be useful; particularly the absence of significant relief following attempted therapeutic interventions.
In the workup of QSS, some conditions have to be ruled out. These include cervical spine pathologies, rotator cuff injuries, referred pain syndromes, and labral injuries [5]. The other important conditions in the differential include brachial plexus pathologies, such as thoracic outlet syndrome and brachial neuritis, suprascapular nerve injury, and glenohumeral joint arthritis [3]. Anterior shoulder dislocation, fracture of the head of the humerus, and blunt trauma can all be sources of axillary nerve injury independent of axillary nerve compression.
Koga et al [28] reported about a patient who presented with QSS symptoms of shoulder pain and upper limb numbness when throwing. The patient was ultimately found to have compression of the axillary nerve between the proximal humerus and the latissimus dorsi tendon. The clinical sequelae can be identical in this situation, but the nerve compression occurs outside of the quadrilateral space.
Imaging and Other Workup
Compression of the axillary nerve may be intermittent and hence imaging of QSS can be challenging. The diagnosis of QSS can be confirmed by imaging [5].
Computed tomography angiography, digital subtraction angiography, and magnetic resonance angiography have all been used to visualize PHCA occlusion [29,30]. There is no “gold standard” diagnostic test for QSS. Magnetic resonance imaging (MRI) is usually the first choice of imaging [31]. MRI can show focal fatty atrophy of the teres minor muscle. It can also exclude pathological causes of shoulder pain [3,31,32]. Arteriography is the cornerstone of diagnosis in QSS. It will reveal compression of the PHCA while the patient’s arm is in abducted and externally rotated [5]. Bilateral upper extremity arteriography is useful in establishing the patient’s baseline healthy anatomy. Decreased outflow from the PHCA would indicate compression of the adjacent axillary nerve [3,5]. In one controlled study, 80% of asymptomatic controls demonstrated PHCA occlusion on arteriography, leading to low specificity [30].
Ultrasound can be used for the diagnosis of QSS. It will show a dilated PHCA and mild atrophy of the deltoid muscle [33]. Occlusion and stenosis of PHCA were detected using ultrasound in another report [14]. Although not so common, teres minor atrophy can also be seen [34,35,36]. Color Doppler sonography has also been used to compare differences in the posterior humeral circumflex arterial flow between provocative and neutral positions [37]. Sonoelastography has also been used in the diagnosis of QSS in patients with axillary schwannoma [38].
Electromyogram (EMG) is also useful in the diagnosis of QSS. The EMG can detect denervation of muscles supplied by the compressed axillary nerve, such as the deltoid and teres minor muscles. The test, however, has a high false-negative rate. In a study by McAdams and Dillingham, four patients with established QSS underwent EMG and MRI testing. They found that all four EMG scans were negative and half of the MRI scans were normal [39]. Although EMG can yield false negative results, it can however eliminate other etiologies of neuropathic pain, such as neurogenic thoracic outlet syndrome.
Treatment
In the literature, there is great variability in the management and treatment of QSS. This is due in part to its recent description and because case reports dominate the literature. The initial treatment is usually conservative. Conservative treatment includes physical therapy and physical activity modification [19]. Physical activity modification can be useful but some patients may find this hard to do. Physical therapy can include transverse friction massage and active release soft tissue massage to the quadrilateral space [5]. Besides therapeutic massage, active shoulder range of motion and scapular stabilization exercises, stretching of the posterior rotator cuff, and the use of nonsteroidal anti-inflammatories have shown success in the treatment of QSS [5]. There has been mild success with the use of ultrasound-guided perineural steroid injections. Pain and other symptomatic relief including tingling, and sensation of coldness following the injection of local anesthetic or steroids can be a diagnostic of QSS. It can also be used with physical therapy for symptomatic treatment [2].
Surgery is considered when patients are unresponsive to conservative treatment for at least six months [40]. Surgical decompression is carried out in such patients. It has proven successful in reversing radial sensory neuropathy secondary to QSS [26]. Since other conditions such effort thrombosis (also known as Paget–Schroetter syndrome) and arterial thoracic outlet syndrome can mimic QSS, imaging and pertinent follow-up testing is essential before planning surgical decompression [41,42]. Despite its lack of specificity, arteriography demonstrating compression of the PHCA and the accompanying presentation of QSS symptoms should raise the suspicion for QSS and surgical decompression may be indicated.
During surgical decompression, the axillary nerve is dissected free to ensure its competency. During the procedure, the axillary nerve and PHCA is palpated while the patient’s arm is placed in external rotation and abduction. This is to verify a freely gliding uncompressed nerve and a consistently strong pulse in the artery [43]. It is also useful to check for fibrous bands around the neurovascular structures, which may be indicative of structural compression [39]. Postoperatively, patients are placed in an arm sling for comfort. Physical therapy is started to prevent the development of adhesions. Physical therapy is an important part of the postoperative recovery [39]. After a successful operation, most athletes can return to their sports [19].
There are several other treatment modalities reported in the literature. These include thrombolysis when there is a thrombus, thrombectomy when there is a distal embolus, aneurysm resection, and endovascular treatment with coiling [44,45,46,47]. In rare instances, quadrilateral space syndrome can resolve spontaneously [48].
Conclusions
QSS is a rare disorder. It can be associated with significant morbidity. Since many symptoms of QSS are nonspecific, there may be a delay in diagnosis and hence delay in treatment. There is one study that showed that the mean interval from the commencement of symptoms to surgical decompression was 14.5 months, with a range from 6–24 months [39]. Medical practitioner awareness of QSS as a differential diagnosis especially in at-risk populations such as athletes, is critical for timely and accurate diagnosis. Careful review of imaging studies is necessary to exclude differential diagnoses, understand etiology, and to devise the best treatment strategy for patients with QSS. Future investigations in patients with QSS could include studies on the prevalence of QSS and a more thorough analysis on the barriers of diagnosis, including limited practitioner awareness of the condition, nonspecific presentation, and the absence of a gold standard workup.
Patients are usually treated conservatively with physical therapy and activity modification. Patients who are non-responsive to conservative therapy after 6 months are subjected to surgery.
References
Cahill B.R., Palmer R.E. Quadrilateral space syndrome. J. Hand Surg. Am. 1983;8:65–69. doi: 10.1016/S0363-5023(83)80056-2.
Flynn L.S., Wright T.W., King J.J. Quadrilateral space syndrome: A review. J. Shoulder Elbow Surg. 2018;27:650–956. doi: 10.1016/j.jse.2017.10.024.
Cothran R.L., Helms C. Quadrilateral space syndrome: Incidence of imaging findings in a population referred for MRI of the shoulder. Am. J. Roentgenol. 2005;184:989–992. doi: 10.2214/ajr.184.3.01840989.
Liveson J.A. Nerve lesions associated with shoulder dislocation; an electrodiagnostic study of 11 cases. J. Neurol. Neurosurg. Psychiatry. 1984;47:742–744. doi: 10.1136/jnnp.47.7.742.
Hoskins W.T., Pollard H.P., McDonald A.J. Quadrilateral space syndrome: A case study and review of the literature. Br. J. Sports Med. 2005;39:e9. doi: 10.1136/bjsm.2004.013367.
Sato T., Tsai T.L., Altamimi A., Tsai T.M. Quadrilateral space syndrome: A case report. J. Hand Surg. Asian Pac. Vol. 2017;22:125–127. doi: 10.1142/S0218810417720108.
McClelland D., Paxinos A. The anatomy of the quadrilateral space with reference to quadrilateral space syndrome. J. Shoulder Elbow Surg. 2008;17:162–164. doi: 10.1016/j.jse.2007.05.013.
Aszmann O.C., Dellon A.L., Birely B.T., McFarland E.G. Innervation of the human shoulder joint and its implications for surgery. Clin. Orthop. Relat. Res. 1996:202–207. doi: 10.1097/ 00003086-199609000-00027.
Brown S.A., Doolittle D.A., Bohanon C.J., Jayaraj A., Naidu S.G., Huettl E.A., Renfree K.J., Oderich G.S., Bjarnason H., Gloviczki P., et al. Quadrilateral space syndrome: The mayo clinic experience with a new classification system and case series. Mayo Clin. Proc. 2015;90:382–394. doi: 10.1016/j.mayocp.2014.12.012.
Durham J.R., Yao J.S., Pearce W.H., Nuber G.M., McCarthy W.J., 3rd Arterial injuries in the thoracic outlet syndrome. J. Vasc. Surg. 1995;21:57–69. doi: 10.1016/S0741-5214(95)70244-X. discussion 70.
Vlychou M., Spanomichos G., Chatziioannou A., Georganas M., Zavras G.M. Embolisation of a traumatic aneurysm of the posterior circumflex humeral artery in a volleyball player. Br. J. Sports Med. 2001;35:136–137. doi: 10.1136/bjsm.35.2.136.
Cirpar M., Gudemez E., Cetik O., Uslu M., Eksioglu F. Quadrilateral space syndrome caused by a humeral osteochondroma: A case report and review of literature. HSS J. 2006;2:154–156. doi: 10.1007/s11420-006-9019-y.
Sanders T.G., Tirman P.F. Paralabral cyst: An unusual cause of quadrilateral space syndrome. Arthroscopy. 1999;15:632–637. doi: 10.1053/ar.1999.v15.015063.
Robinson P., White L.M., Lax M., Salonen D., Bell R.S. Quadrilateral space syndrome caused by glenoid labral cyst. AJR Am. J. Roentgenol. 2000;175:1103–1105. doi: 10.2214/ajr. 175.4.1751103.
Mohandas Rao K.G., Somayaji S.N., Ashwini L.S., Ravindra S., Abhinitha P., Rao A., Sapna M., Jyothsna P. Variant course of posterior circumflex humeral artery associated with the abnormal origin of radial collateral artery: Could it mimic the quadrangular space syndrome? Acta Med. Iran. 2012;50:572–576.
Pires L.A.S., Souza C.F.C., Teixeira A.R., Leite T.F.O., Babinski M.A., Chagas C.A.A. Accessory subscapularis muscle—A forgotten variation? Morphologie. 2017;101:101–104. doi: 10.1016/j.morpho. 2017.04.003.
Nishimura M., Kobayashi M., Hamagashira K., Noumi S., Ito K., Kato D., Shimada J. Quadrilateral space syndrome: A rare complication of thoracic surgery. Ann. Thorac. Surg. 2008;86: 1350–1351. doi: 10.1016/j.athoracsur.2008.02.039.
Koga R., Furushima K., Kusano H., Hamada J., Itoh Y. Quadrilateral space syndrome with involvement of the tendon of the latissimus dorsi. Orthopedics. 2017;40:e714–e716. doi: 10.3928/01477447-20170117-06.
Van de Pol D., Kuijer P.P., Langenhorst T., Maas M. High prevalence of self-reported symptoms of digital ischemia in elite male volleyball players in the Netherlands: A cross-sectional national survey. Am. J. Sports Med. 2012;40:2296–2302. doi: 10. 1177/0363546512456973.
McClelland D., Hoy G. A case of quadrilateral space syndrome with involvement of the long head of the triceps. Am. J. Sports Med. 2008;36:1615–1617. doi: 10.1177/0363546508321476.
Cummins C.A., Schneider D.S. Peripheral nerve injuries in baseball players. Neurol. Clin. 2008;26:195–215. doi: 10.1016/j.ncl. 2007.11.014.
Aval S.M., Durand P., Jr., Shankwiler J.A. Neurovascular injuries to the athlete’s shoulder: Part II. J. Am. Acad. Orthop. Surg. 2007;15:281–289. doi: 10.5435/00124635-200705000-00006.
De Mooij T., Duncan A.A., Kakar S. Vascular injuries in the upper extremity in athletes. Hand Clin. 2015;31:39–52. doi: 10.1016/j.hcl.2014.09.004.
Monteleone G., Gismant M., Stevanato G., Tiloca A. Silent deltoid atrophy in beach volleyball players: A report of two cases and literature review. Int. J. Sports Phys. Ther. 2015;10:347–353.
Rollo J., Rigberg D., Gelabert H. Vascular quadrilateral space syndrome in 3 overhead throwing athletes: An underdiagnosed cause of digital ischemia. Ann. Vasc. Surg. 2017;42:63e1–63e6. doi: 10.1016/j.avsg.2016.10.051.
Brown D.L., Chung K.C. Quadrangular space syndrome associated with superficial radial sensory neuropathy. Ann. Plast. Surg. 1999;43:207–210.
Jackson M.R. Upper extremity arterial injuries in athletes. Semin. Vasc. Surg. 2003;16:232–239. doi: 10.1016/S0895-7967(03)00029-2.
Koga R., Furushima K., Kusano H., Hamada J., Itoh Y. Quadrilateral space syndrome with involvement of the tendon of the latissimus dorsi. Orthopedics. 2017;40:e714–e716. doi: 10.3928/01477447-20170117-06.
Chautems R.C., Glauser T., Waeber-Fey M.C., Rostan O., Barraud G.E. Quadrilateral space syndrome: Case report and review of the literature. Ann. Vasc. Surg. 2000;14:673–676. doi: 10. 1007/s100169910120.
Mochizuki T., Isoda H., Masui T., Ohkawa Y., Takahashi M., Takehara Y., Ichijo K., Kodaira N., Kitanaka H. Occlusion of the posterior humeral circumflex artery: Detection with MR angiography in healthy volunteers and in a patient with quadrilateral space syndrome. AJR Am. J. Roentgenol. 1994;163:625–627. doi: 10.2214/ajr.163.3.8079857.
Chen H., Narvaez V.R. Ultrasound-guided quadrilateral space block for the diagnosis of quadrilateral syndrome. Case Rep. Orthop. 2015;2015:378627. doi: 10.1155/2015/378627.
Chen D., Cai P., Lao G., Gu Y. Quadrilateral space syndrome. Chin. Med. J. 1995;108:109–112.
Feng S.-H., Hsiao M.-Y., Wu C.-H., Özçakar L. Ultrasound-guided diagnosis and management for quadrilateral space syndrome. Pain Med. 2017;18:184–186. doi: 10.1093/pm/pnw256.
Wilson L., Sundaram M., Piraino D.W., Ilaslan H., Recht M.P. Isolated teres minor atrophy: Manifestation of quadrilateral space syndrome or traction injury to the axillary nerve? Orthopedics. 2006;29:447–450.
Lopez Ovenza J.M., Ranalletta M., Alonso Hidalgo I., Tanoira I., Bongiovanni S., Maignon G. Quadrilateral space syndrome with compromise of the teres minor muscle. Medicina. 2011;71:49.
Molina Granados J.F., Dominguez Franjo E. Quadrilateral space syndrome with complete denervation of the deltoid and teres minor muscles. Radiologia. 2010;52:373–374. doi: 10.1016/j.rx. 2010.03.009.
Brestas P.S., Tsouroulas M., Nikolakopoulou Z., Malagari K., Drossos C. Ultrasound findings of teres minor denervation in suspected quadrilateral space syndrome. J. Clin. Ultrasound. 2006;34:343–347. doi: 10.1002/jcu.20239.
Hung C.Y., Chang K.V., Chen P.T., Ho Y.T., Han D.S., Chen W.S., Wang T.G. Sonoelastography for the evaluation of an axillary schwannoma in a case of quadrilateral space syndrome. Clin. Imaging. 2014;38:360–363. doi: 10.1016/j.clinimag.2013.12.019.
McAdams T.R., Dillingham M.F. Surgical decompression of the quadrilateral space in overhead athletes. Am. J. Sports Med. 2008;36:528–532. doi: 10.1177/0363546507309675.
Manske R.C., Sumler A., Runge J. Quadrilateral space syndrome. Hum. Kinet. 2009;14:45–47. doi: 10.1123/att.14.2.45.
Reeser J.C. Diagnosis and management of vascular injuries in the shoulder girdle of the overhead athlete. Curr. Sports Med. Rep. 2007;6:322–327.
Hangge P., Rotellini-Coltvet L., Deipolyi A.R., Albadawi H., Oklu R. Paget-schroetter syndrome: Treatment of venous thrombosis and outcomes. Cardiovasc. Diagn. Ther. 2017;7:S285–S290. doi: 10.21037/cdt.2017.08.15.
Francel T.J., Dellon A.L., Campbell J.N. Quadrilateral space syndrome: Diagnosis and operative decompression technique. Plast. Reconstr. Surg. 1991;87:911–916. doi: 10.1097/00006534- 199105000-00016.
Reekers J.A., den Hartog B.M., Kuyper C.F., Kromhout J.G., Peeters F.L. Traumatic aneurysm of the posterior circumflex humeral artery: A volleyball player’s disease? J. Vasc. Interv. Radiol. 1993;4:405–408. doi: 10.1016/S1051-0443(93)71888-6.
Duwayri Y.M., Emery V.B., Driskill M.R., Earley J.A., Wright R.W., Paletta G.A., Jr., Thompson R.W. Positional compression of the axillary artery causing upper extremity thrombosis and embolism in the elite overhead throwing athlete. J. Vasc. Surg. 2011;53: 1329–1340. doi: 10.1016/j.jvs.2010.11.031.
Arko F.R., Harris E.J., Zarins C.K., Olcott C.T. Vascular complications in high-performance athletes. J. Vasc. Surg. 2001; 33:935–942. doi: 10.1067/mva.2001.115162.
Reekers J.A., Koedam N. Volleyball-related ischemia of the hand. Cardiovasc. Interv. Radiol. 1998;21:261. doi: 10.1007/ s002709900259.
Gregory T., Sangha H., Bleakney R. Spontaneous resolution of quadrilateral space syndrome: A case report. Am. J. Phys. Med. Rehabil. 2015;94:e1–e5. doi: 10.1097/PHM.0000000000000237.
No comments:
Post a Comment