Blount Disease
Dr. KS Dhillon
Introduction
Blount disease was first described by Walter Putnam Blount in 1937.
Blount disease is also known as tibia vara. It is an acquired genu varus deformity in children. It is caused by disruption of the normal cartilage growth at the proximal medial metaphysis of the tibia. This disease develops due to excessive compressive forces on the medial aspect of the proximal tibial physis. These forces lead to altered enchondral bone formation. Blount disease can be either unilateral or bilateral. It manifests in 2 forms i.e. infantile and adolescent. It is distinguished by variations in age of onset and presentation. The infantile or early-onset form is usually bilateral. It typically presents in children between the ages of 1 and 5 years. It tends to exacerbate after the initiation of walking. The adolescent form manifests itself at a later stage. It may be unilateral or bilateral.
The precise pathophysiology of the condition remains unclear. Obesity, early walking, and African-American heritage are recognized as risk factors for developing Blount disease. The severity of the disease can vary from articular cartilage irregularities to limb length discrepancies (1). Depending on the age and severity at presentation the treatment of Blount disease can vary from bracing to surgical interventions. The treatment options include knee-ankle-foot orthoses (KAFOs), hemiepiphysiodesis, and corrective proximal tibial osteotomies.
Radiographic findings are diagnostic. The Langenskiöld classification system describes the 6 radiographic stages of Blount disease.
Etiology
Blount disease has a multifactorial etiology. Both biological and mechanical factors are involved. Mechanical overloading of the proximal tibia is a significant contributor, especially in children who are overweight and start walking early. It is however not the sole cause of the condition. The infantile form also affects normal-weight children. The infantile form and the higher prevalence among African-American patients indicate a potential hereditary component. Besides mechanical overload, genetic susceptibility is also implicated in the development of Blount disease.
Epidemiology
The prevalence of Blount disease in the USA is less than 1%. The infantile form is most common. It is more prevalent in males than females. In 80% of cases, infantile Blount disease is bilateral. Adolescent Blount disease is also known as adolescent genu varum. It is generally less severe and more likely to be unilateral. This disease is most prevalent among children of Scandinavian and African ancestry.
Pathophysiology
Blount disease is caused by growth inhibition that is induced by excessive compressive forces. The compressive forces lead to cartilage damage and a subsequent delay in ossification. The mechanical overload leads to alteration in enchondral bone formation. When the compressive forces peak at the posteromedial aspect of the physis, there is heightened growth inhibition on the medial side of the knee. This leads to the development of a continual varus deformity (2).
Clinical Presentation
Genu varum is a normal finding in children below the age of 2 years. After that alignment transitions to valgus, reaching its peak around the age of 3 years. Persistent genu varum often serves as the initial indicator for diagnosis in children who are young and overweight (3). As this growth disorder progresses, knee deformities and associated abnormalities gradually worsen. This results in a 3-dimensional deformity that combines varus, internal tibial rotation, procurvatum, and limb length discrepancy.
Infantile Blount Disease
Infantile Blount disease is usually seen in children between the ages of 1 and 3 years. It is usually bilateral and is characterized by varus deformity of the tibia and internal tibial torsion. Pain is usually uncommon. A palpable "beak" may be present over the medial aspect of the proximal tibial condyle.
There is a lateral thrust at the knee indicating lateral translation of the knee joint during weight-bearing. Irreversible asymmetric medial proximal tibial epiphysiodesis usually develops around the ages of 6 to 8 years. This makes conservative treatments ineffective.
Adolescent Blount Disease
Adolescent Blount disease usually develops in children in their late childhood or early adolescence. It is often accompanied by pain in the medial aspect of the knee. This disease is usually associated with being obese or overweight. The presentation of the disease is usually unilateral. There may be associated abnormalities of the distal femur.
Evaluation
History, physical examination, and plain X-rays are sufficient to diagnose Blount disease. In the initial stages, a long-leg anteroposterior radiograph is used to measure the varus. For accurate measurement a bilateral projection of the radiograph from the hip to the ankle is necessary.
Indicators of Blount Disease
Findings suggestive of Blount disease include:
Medial beaking of the epiphysis
Irregular ossification
Medial slope of the epiphysis
Widened and irregular medial physis
Metaphysis in varus
Angles For Blount Disease Detection
Specific angle measurements are carried out to detect Blount disease in children. There are various angles, such as the Levine-Drennan angle, that are used to assess the relationship between the tibia shaft and its upper growth plate. An angle exceeding 11° indicates the presence of Blount disease. The angles for detection of Blount disease include:
1. Metaphyseal-diaphyseal angle (MDA): This angle can predict the progression of Blount disease. The intersection occurs between a line drawn from the most distal point on the lateral and medial beaks of the tibial metaphysis to a line perpendicular to the long axis of the tibial diaphysis (4,5).
The disease progression can be predicted as follows:
An angle of more than 16° is associated with a 95% risk of deformity progression (4,5).
An angle of less than 10° is likely physiological, with a 95% chance of spontaneous resolution (4,5).
An angle between 11° and 16° needs close observation for potential tibia vara progression (4,5).
The angular abnormalities include intra- and extra-articular varus malalignment, distal tibial valgus, lateral and medial laxity, internal tibial rotation, procurvatum, and distal femoral deformities (4,5).
2. Tibiofemoral angle: The tibiofemoral angle measures the severity of the varus deformity of the knee.
3. Medial metaphyseal beak angle: The medial metaphyseal beak angle (MMBA) is a potential diagnostic screening tool for patients at risk of Blount disease. When combined with the MDA, MMBA can confirm the diagnosis. This results in earlier diagnosis and improved patient outcomes.
Magnetic resonance imaging (MRI) assesses the menisci, cartilage, ligaments, and vascularity of the physis. The MRI outperforms X-rays in detecting cartilaginous changes (6). Gadolinium-enhanced MRI is useful for pediatric patients with neglected or delayed forms of Blount disease observed after the age of 4 years but before the development of radiographic epiphysiodesis.
Langenskiöld Classification
Langenskiöld classified Blount disease into 6 stages. The stages indicate an increase in severity and medial physeal collapse. The staging is specifically applied to the infantile form. A physeal bar becomes evident from stage V onward. This occurs due to an injury or infection which causes disruption of normal cartilage in a growing physis. The healing process involves bone and not the cartilage. In skeletally immature children the physeal bars cause angular deformities and limb length discrepancies. MRI-based classifications, such as Fort-de-France (FDF), have become more prevalent recently. The x-ray-based classification however remains most widely used (7).
Stages of ligament laxity: There are 4 recognized stages of ligament laxity. These include:
Stage 0: Normal laxity
Stage +: Medial laxity
Stage ++: Lateral laxity
Stage +++: Multidirectional laxity
Langenskiöld classification system: There are 6 stages of the Langenskiöld classification system (Fig 1). These include (7,8):
Stage I: Irregularity of metaphyseal zone
Stage II: Medial metaphyseal beaking
Stage III: Development of "step" in the metaphyseal beak
Stage IV: Epiphysis beaking that occupies a pit in the medial metaphysis
Stage V: Double epiphyseal plate
Stage VI: Bony bar formation
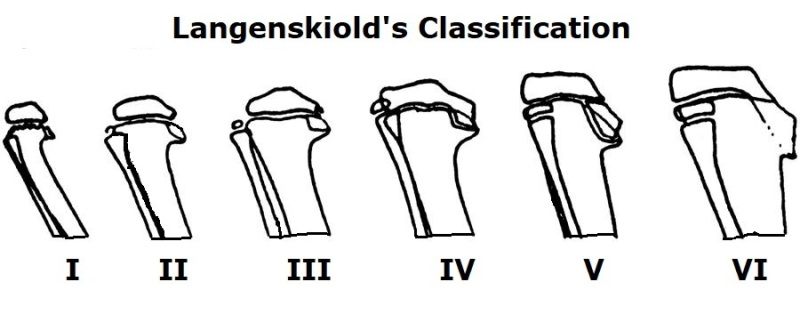
Fig 1
Management
The treatment of Blount's disease depends on the age of the child and severity of the deformity. The discrepancy between skeletal age and chronological age diminishes as the chronological age increases. A preoperative assessment of skeletal age is crucial as it can affect the timing and magnitude of the correction. When surgery is indicated, the surgical intervention aims to restore normal joint and limb alignment, achieve equal limb lengths at skeletal maturity, and prevent recurrence.
Brace
Children below the age of 4 years with Langenskiöld stage I or II disease
can be treated with KAFOs. The brace extends from the upper thigh to the foot and it applies valgus force to the knee. Orthotic treatment is successful when initiated before the age of 3 years in non-obese children who primarily wear the brace at night. The treatment continues for 1 year. In cases where orthoses do not prove effective, osteotomy has to be considered before age 4 when indicated. Fitting a brace on a boisterous child younger than 3 years of age poses a significant challenge that can affect treatment (9). Eighty percent of pediatric patients with progressive early-onset Blount disease undergoing surgical axis realignment before age 4 achieve a full recovery. The emergence of lateral thrust during weight-bearing indicates the onset of mechanical knee failure.
Guided Growth
Guided growth is obtained by hemiepiphysiodesis. It involves a surgical technique to correct angular limb deformities in skeletally immature patients. It is a good alternative to corrective osteotomies. Hemiepiphysiodesis is cost-effective, reduces pain for patients, immobilization times are shorter, and surgical risks are diminished.
The most commonly performed procedure is hemiepiphysiodesis of the lateral epiphysis with extraperiosteal implants such as pins, staples, or tension band plating. Bone growth stops or slows down on the side of epiphysiodesis. The growth plate on the other side continues to grow normally and it gradually straightens the bone over time. The advantage of this approach is that the entire physis can resume growth after the hardware is removed.
For this procedure to be successful the child should have at least 4 years of growth. The basis of this treatment modality is the Hueter-Volkmann principle, which posits that compression inhibits longitudinal growth.
Unlike genu varum associated with other disorders, the outcome of guided growth in Blount disease is less predictable. This is potentially due to the involvement of the diseased proximal medial physis. In a study by Schroerlucke et al 8 hardware failures occurred in 18 Blount disease extremities representing a failure rate of 44% (10). Use of two parallel plates or non-cannulated solid stainless steel screws are recommended for patients with moderate-to-severe Blount disease (11). Hemiepiphysiodesis and guided-growth systems are viable options for individuals with late-onset Blount disease who present with a varus deformity of less than 15°, limb shortening not exceeding 1 cm, and having at least 2 years of skeletal growth. Surgical intervention is not appropriate for children 2 years and younger (12).
Osteotomy
In pediatric patients with documented and progressive Blount disease or FDF stage I who demonstrate risk factors, realignment osteotomy is typically performed before the age of 4 years (13). Due to high recurrence rate in infantile Blount disease, overcorrection osteotomies to achieve between 5º and 15° of valgus are necessary. There has to be lateral translation, 10° to 15° of lateral derotation, and 5° to 10° of valgus.
There are various osteotomy techniques described for Blount disease. These include opening and closing wedges, serrations, domes, opening wedges, and inclined osteotomies. The correction can be acute or gradual.
Gradual correction produces a more precise mechanical axis and correction of leg length discrepancy. A systematic review by Feldman et al comparing acute versus gradual correction for Blount disease showed that gradual deformity correction is a more accurate treatment method of tibia vara than acute correction. No difference in the reoperation rate existed between the 2 procedures (14). With acute correction of the tibia vara, there is a risk of peroneal nerve injury and compartment syndrome regardless of the kind of osteotomy and fixation method used (15).
Acute Correction
The varus distal fragment is fixed in translation and external rotation to correct the internal rotation deformity during acute correction. Other surgical procedures that are necessary, such as medial plateau elevation and physeal bar resection, are carried out concurrently with the osteotomy. Hemiepiphysiodesis is appropriate if the bar is more than 50% of the size of the physis. The osteotomy level is positioned below the tibial tuberosity to prevent patella baja. Patella baja can lead to extensor insufficiency and knee pain.
Regardless of the stage of the disease, children who are 3 years or older, and patients with stage III Blount disease, irrespective of age, are considered suitable for an osteotomy. It can be challenging to accurately measure limb alignment after acute or gradual correction. Some researchers utilize intraoperative fluoroscopy with the electrocautery cord placed across the skin, overlaying the center of the hip and ankle to visualize mechanical axis alignment (16).
With acute correction, the deformity can be immediately corrected. This approach, however, increases the risk of compartment syndrome and peroneal nerve injury due to acute lengthening.
Gradual Correction
For gradual correction, an osteotomy is performed, and a frame is attached to enable progressive correction. Two commonly used devices include the Ilizarov Ring External Fixator or the Taylor Spatial Frame. Typically a treatment duration of 12 to 18 weeks is required. With gradual correction, the risk of neurovascular compromise and compartment syndrome is minimized while allowing for correction of deformity in all planes. A potential drawback is pin site infection.
Asymmetrical Physeal Distraction
Asymmetrical physeal distraction is a procedure that is rarely used. For asymmetrical physeal distraction 2 half-pins of 6 mm are inserted into the proximal tibial epiphysis and 2 pins into the diaphysis. Progressive distraction is then done at a rate of 1.5 mm per day. With the monolateral fixator, an average of 13° of angular correction can be obtained. This procedure is not so popular due to risks of septic arthritis, discomfort during distractions, and the potential for premature closure of the growth plate (17).
Physeal Bar Resection
Surgical resection is difficult because there is no distinct region of osseous tether in patients with Blount disease. Physeal bar resection aims to restore normal growth and prevent further deformity. There are improved outcomes in children who receive physeal bar resection or epiphysiolysis before the age of 7 years, combined with a valgus osteotomy. Children aged 7 years and older are not suitable for this surgery. Epiphysiolysis as a standalone procedure has minimal use in these patients (18,19).
Medial Tibial Plateau Elevation
Progression of Blount disease can lead to lateral tibial translation and entry of the medial femoral condyle into the posteromedial depression. This can lead to a varus thrust gait. Children 6 years and older with severe Blount disease, at Langenskiöld stage V or VI, who exhibit a substantial posterior depression of the medial tibial plateau are suitable candidates for posteromedial tibial plateau elevation. To preserve the medial tibial plateau surgeons recommend conducting an intraepiphyseal or transepiphyseal osteotomy that hinges on the articular cartilage of the intercondylar notch. The aim should be to simultaneously correct the posterior depression of the medial plateau by incorporating a larger portion of the graft. To prevent the recurrence of a varus thrust gait, there is a need to perform lateral proximal tibial and fibular epiphyseodesis concurrently (20,21).
Differential Diagnosis
It can be challenging to distinguish infantile tibia vara from physiological bowing of the legs. In patients with physiological bowing, there is gradual curve development of both the tibia and femur. The proximal tibial bowing in Blount disease is acute. An MDA of more than 11° is indicative of Blount disease.
Other differential diagnoses include:
Rickets
Metaphyseal chondrodysplasia
Ollier disease
Proximal tibial physeal injury resulting from trauma, radiation, or infection Osteomyelitis
Thrombocytopenia absent radius syndrome
In Blount disease, there is asymmetrical beaking and sharp angular deformities, which are usually absent in rickets. The presence of multiple enchondromas indicates the existence of Ollier disease (22,23).
Prognosis
The prognosis for Blount disease depends on the age of the individual and also on the severity of the disease at the time of presentation. Infantile Blount disease usually has a favorable prognosis. There is a low deformity recurrence rate when the disease is treated early. Complete or partial regression can be achieved in patients in the early stages of the disease. Those in the later stages will most likely progress without early intervention. If left untreated, patients with the late-onset form of the disease may experience progression and significant joint deformity (24).
Complications
Complications associated with the treatment of Blount disease can be due to the disease itself or due to operative treatment.
The operative complications include:
Vascular impairment
Wound infection
Pathologic fractures
Malalignment
Complications of the disease include (24):
Recurrence of deformity
Joint degeneration in the long-term
Adulkasem et al (25) in a retrospective cohort study of 58 patients with infantile Blount disease (101 extremities) who underwent tibial osteotomy found the following factors to be predictive of recurrence:
Age less than 42 months
LaMont classification type C
Medial metaphyseal beak angle of more than 128º
Conclusion
The initial treatment of Blount’s disease is leg bracing for patients below the age of 3 years. Surgery is often recommended if the deformity is not corrected before the age of 4 years and in patients with Langenskiӧld stage III or greater disease. For surgical correction of Blount’s disease, metaphyseal osteotomy remains a foundational treatment option. Many surgical techniques have been developed and used for the treatment of Blount’s disease. The best treatment for this disease, which can be accompanied by the best functional outcomes depends on the patient’s age, the severity of the deformity, psychosocial factors, and the experience of the doctor doing the treatment.
References
Janoyer M. Blount disease. Orthop Traumatol Surg Res. 2019 Feb;105(1S):S111-S121.
LANGENSKIOLD A. Aspects of the pathology of tibia vara (osteochondrosis deformans tibiae). Ann Chir Gynaecol Fenn. 1955;44(1):58-63.
Sabharwal S. Blount disease: an update. Orthop Clin North Am. 2015 Jan;46(1):37-47.
Davids JR, Blackhurst DW, Allen BL. Radiographic evaluation of bowed legs in children. J Pediatr Orthop. 2001 Mar-Apr;21(2):257-63.
Park BK, Park KB, Kwak YH, Jin S, Kim HW, Park H. A comparative evaluation of tibial metaphyseal-diaphyseal angle changes between physiologic bowing and Blount disease. Medicine (Baltimore). 2019 Apr;98(17):e15349.
Gill KG, Nemeth BA, Davis KW. Magnetic resonance imaging of the pediatric knee. Magn Reson Imaging Clin N Am. 2014 Nov;22(4):743-63.
Erkus S, Turgut A, Kalenderer O. Langenskiöld Classification for Blount Disease: Is It Reliable? Indian J Orthop. 2019 Sep-Oct; 53(5):662-664.
Vosoughi F, Nabian MH, Simon AL, Aghaghazvini L, Zargarbashi R, Yekaninejad MS. Langenskiöld classification of tibia vara: a multicenter study on interrater reliability. J Pediatr Orthop B. 2022 Mar 01;31(2):114-119.
Sabharwal S, Sabharwal S. Treatment of Infantile Blount Disease: An Update. J Pediatr Orthop. 2017 Sep;37 Suppl 2:S26-S31.
Schroerlucke S, Bertrand S, Clapp J, Bundy J, Gregg FO. Failure of Orthofix eight-Plate for the treatment of Blount disease. J Pediatr Orthop. 2009 Jan-Feb;29(1):57-60.
Stitgen A, Garrels K, Kobayashi H, Vanderby R, McCarthy JJ, Noonan KJ. Biomechanical comparison between 2 guided-growth constructs. J Pediatr Orthop. 2012 Mar;32(2):206-9.
Sabharwal S. Blount disease. J Bone Joint Surg Am. 2009 Jul;91(7):1758-76.
Griswold B, Gilbert S, Khoury J. Opening Wedge Osteotomy for the Correction of Adolescent Tibia Vara. Iowa Orthop J. 2018;38:141-146.
Feldman DS, Madan SS, Ruchelsman DE, Sala DA, Lehman WB. Accuracy of correction of tibia vara: acute versus gradual correction. J Pediatr Orthop. 2006 Nov-Dec;26(6):794-8.
Loder RT, Johnston CE. Infantile tibia vara. J Pediatr Orthop. 1987 Nov-Dec;7(6):639-46.
S DMTS, Taqi M, De Leucio A. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Jan 9, 2024. Blount Disease.
de Pablos J, Franzreb M. Treatment of adolescent tibia vara by asymmetrical physeal distraction. J Bone Joint Surg Br. 1993 Jul;75(4):592-6.
LANGENSKIOELD A, RISKA EB. TIBIA VARA (OSTEOCHONDROSIS DEFORMANS TIBIAE): A SURVEY OF SEVENTY-ONE CASES. J Bone Joint Surg Am. 1964 Oct;46:1405-20.
Andrade N, Johnston CE. Medial epiphysiolysis in severe infantile tibia vara. J Pediatr Orthop. 2006 Sep-Oct;26(5):652-8.
van Huyssteen AL, Hastings CJ, Olesak M, Hoffman EB. Double-elevating osteotomy for late-presenting infantile Blount's disease: the importance of concomitant lateral epiphysiodesis. J Bone Joint Surg Br. 2005 May;87(5):710-5.
Accadbled F, Laville JM, Harper L. One-step treatment for evolved Blount's disease: four cases and review of the literature. J Pediatr Orthop. 2003 Nov-Dec;23(6):747-52.
Bhattacharjee R, Chakraborty PP, Roy A, Biswas SN. Blount's disease: a rickets mimicker. BMJ Case Rep. 2016 May 13;2016.
Birch JG. Blount disease. J Am Acad Orthop Surg. 2013 Jul;21(7):408-18.
Doyle BS, Volk AG, Smith CF. Infantile Blount disease: long-term follow-up of surgically treated patients at skeletal maturity. J Pediatr Orthop. 1996 Jul-Aug;16(4):469-76.
Adulkasem N, Wongcharoenwatana J, Ariyawatkul T, Chotigavanichaya C, Eamsobhana P. A Predictive Score for Infantile Blount Disease Recurrence After Tibial Osteotomy. J Pediatr Orthop. 2023 Apr 1. 43 (4):e299-e304.
No comments:
Post a Comment