Total Knee Arthroplasty Periprosthetic Fracture
Dr. KS Dhillon
Introduction
The number of individuals with joint arthroplasty is steadily growing. This is due to the fact that the population is continuously increasing and getting older on one hand, and on the other hand there is demand for high physical performance even at an advanced age. The Endoprostheses Register in Germany in 2018 recorded a total of over 300,000 implantations or revisions of artificial joints. More than 132,000 of these involved the knee joint. Kurtz et al (1) projected that 3.48 million knee arthroplasties will be done in the USA in 2030. With the increasing number of implanted artificial joints, the number of complications will naturally also rise. A major complication is a periprosthetic fracture which has massive socioeconomic consequences. The incidence of periprosthetic fractures is low after primary TKA but the risk increases after revision surgery. Several factors have to be taken into account when treating a periprosthetic fracture. Basic principles of classical fracture management can rarely be applied to periprosthetic fracture management since the biomechanics and bone healing are significantly altered in the presence of an artificial joint. Identifying the cause of the fracture is a key element in determining further treatment. The strategy is significantly affected by the presence of a prosthetic joint infection, aseptic loosening, or a pathological fracture in malignant disease. Since unexpected findings sometimes first manifest themselves intraoperatively, surgical treatment is recommended in a specialized center.
Epidemiology
The causes of periprosthetic fractures around TKA are diverse. Besides age, gender, the time elapsed since implantation and revision surgery also have an influence on fracture risk (2). The incidence of a periprosthetic fracture after primary TKA is about 2%. In the case of revision surgery, the incidence increases by up to 38%. The most common site for fracture is the femur, followed by the patella and tibia (3,4,5). High-energy trauma is a rare cause of these fractures. Often, the fracture is preceded by low-energy trauma in patients with general risk factors such as osteoporosis, prosthetic joint infection (PJI), or aseptic loosening of the implants. The treatment depends on the underlying risk factor for the fracture. The periprosthetic fractures can occur intraoperatively or postoperatively. If intraoperative fractures are detected during implantation, they can be treated then and there. In the case of postoperative fractures, the fracture's cause and the components' fixation must be considered to decide whether the implant can be retained or has to be replaced. The required information can be obtained from a detailed medical history and corresponding diagnostics.
Diagnosis
The exact medical history is of great importance for further treatment. If after TKR the patient was never free of symptoms in the area of the affected knee joint, the focus is on PJI, incorrect positioning, or intraoperatively missed periprosthetic fractures. It may be a pathological fracture if the patient suffers from a malignant disease or osteoporosis. The diagnosis is made by doing x-rays of the affected knee joint in two perpendicular planes (anterior-posterior and lateral) and an axial image of the patella. For further planning any implants or prostheses of the neighboring joints must also be displayed. If the pain level and general condition of the patient permits, an x-ray of the whole lower limb is taken to identify axial deviations. A comparison with preexisting imaging if present allows conclusions to be drawn about loosening of the implants, peri-implant osteolysis, or malposition of the components (6). CT imaging can detect non-displaced and X-ray occult fractures. It can help to determine the fracture morphology and bone quality. Rotational malposition of the components can be effectively assessed with CT. In direct proximity to inserted implants, the validity of CT can be limited through metal-related interference artifacts. In exceptional cases, an MRI can provide valuable additional information about the soft tissue envelope, occult fractures, the bone-prosthesis interface, and bone cement (7). Information on bone quality can be obtained by performing a DEXA absorptiometry. This information is used when planning the procedure and selecting implants. If the medical history, imaging, or laboratory tests indicate a PJI, the affected knee joint must be biopsied. The detection or exclusion of a PJI is particularly important because further procedures significantly depend on it.
Treatment
Distal femur
TKR periprosthetic fractures occur most frequently in the distal femur. The incidence of such fractures is between 0.3% to 2.5% (6). This area is particularly at risk due to the large moments of force that occur in the supracondylar region in patients with low-energy trauma. The Lewis and Rorabeck classification divides distal femoral fractures into 3 types depending on the degree of dislocation and the fixation of the components (Fig. 1). It is well established in clinical practice (8). In type 1 and 2 fractures the components are fixed and they differ only in the degree of dislocation. The results of surgery with nonlocking osteosyntheses were inferior to those of conservative treatment.
With the introduction of locking plate systems by the AO Foundation in 2000, the results of plate osteosyntheses in supracondylar periprosthetic femoral fractures were good (9,10,11,12). In 2005 the AO Foundation developed special periprosthetic fracture plates that met the mechanical and geometric requirements for treating this kind of fractures even better (13). If the locking mechanism is polyaxially, some of the locking head screws can be placed in the distal fragment without collision with the femoral prosthetic component, even in patients with very distal fractures. Insertion of screws in 8 to 10 cortices above and below the fracture is recommended (3). In patients with an intramedullary implant, extra short screws can be inserted monocortically. It is possible to insert several screws into the bone passing intramedullary implants by using additional modules such as the locking adapting plate, which is screwed onto the plate. Too rigid fixation by plate osteosynthesis has to be avoided so as not to compromise bone healing. By using long plates load sharing can be improved.
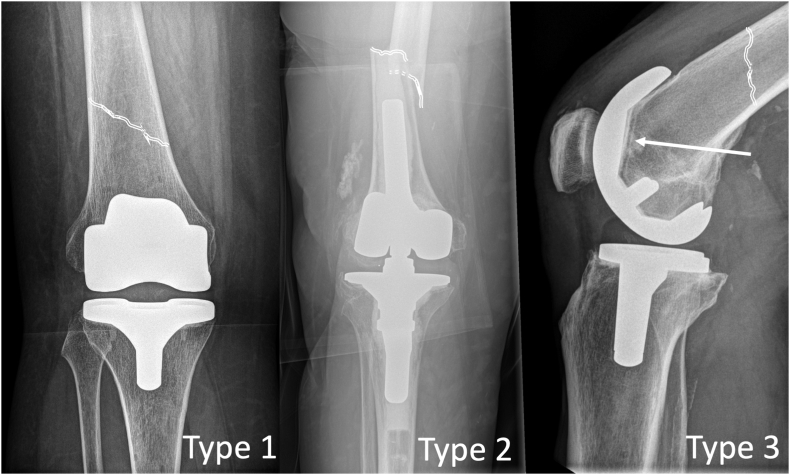
Fig 1
The screws should not be placed too close to the fracture site to avoid stress risers (14). Since there is high mechanical load with implants that are already in place, the use of broad and therefore more stable plates, is recommended especially in comminuted fractures to prevent implant failure. If the patient is fit for surgery, surgical treatment with locking plate osteosynthesis should be performed to reduce complications such as non-union. Postoperative exercises can prevent stiffening of the knee joint. Conservative treatment requires the affected extremity to be immobilized across the knee joint for a longer period which leads to knee stiffness (15). Retrograde intramedullary nail osteosynthesis can be done depending on the prosthesis model and taking into account ipsilateral femoral implants. Retrograde intramedullary nail osteosynthesis has lost much of its importance as it is inferior to locking plate osteosynthesis with regards to stability, non-union, and revision procedures. The advantages of intramedullary nailing are less invasiveness and the resulting lower infection rate and less blood loss. For a retrograde intramedullary nailing osteosynthesis, several conditions must be met. The femoral component of the TKA must have an open-box design. The thickest part of the nail must be able to pass through the open intercondylar space during insertion. The prosthesis model must be known. It is important to remember that the nail diameter is usually given for the part of the nail that is diaphyseal in the area of the isthmus. The distal nail end, which has to fit through the intercondylar space of the prosthesis, usually has a larger diameter. For safe nail entry, the affected knee joint must be able to flex at least 60°. Very distal fractures are not suitable for intramedullary nail osteosynthesis because at least 2 locking screws have to be placed in the distal fragment (16,17). Retrograde intramedullary nail osteosynthesis for the treatment of periprosthetic distal femoral fractures around TKA is reserved for situations where there are contraindications for plate osteosynthesis. In all other cases, locking plate osteosynthesis should be carried out.
There is no comminuted zone in Type 1 fractures. The dislocation in such fractures is a maximum of 5 mm with the axial deviation a maximum of 5° (18). High degree of instability is not present. A lateral locking plate osteosynthesis is the osteosynthesis procedure of choice.
An insertion guide via soft tissue-sparing approaches in the region of the lateral femur can be used to insert modern systems. The proximal screw holes are approached through small incisions. These kinds of fractures rarely require direct exposure.
A dislocation of more than 5 mm or an axial deviation of more than 5° is referred to as a type 2 fracture. Compared to type 1 fractures, the stability in type 2 fractures is reduced due to the dislocation. In multifragmentary situations with interposed soft tissue, it is often necessary to expose and reduce the fracture. The reduction can be secured with a cerclage wire. When the femoral component does not have a box, the distal fixation of the osteosynthesis is usually not affected. Even in the presence of a box as in varus-valgus-constrained or PS-implants and relatively proximal fracture, a sufficient number of screws can be placed distally. In both of these cases, the single lateral locking plate osteosynthesis is used. If the fracture is far distal and the femoral component has a box or a stem, the distal fixation can be significantly compromised. To stabilize the medial column additional medial plate osteosynthesis and insertion of supplemental distal screws is recommended. This increases the stability of the osteosynthesis (19,20). After knee replacement, the morbidity of the approach for performing medial plate osteosynthesis is a challenge for surgeons since at least two approaches are already present due to the implantation of the prosthesis and the insertion of the lateral plate. The iatrogenic trauma to soft tissues should be kept as small as possible to avoid compromising fracture healing. In this situation, the use of a helix plate is a stable and minimally invasive procedure. For this, a straight locking plate is torqued about 90° to 120° in the axial direction and then bent according to the anatomy of the individual femur. Using a small medial approach in the area of the distal femur, the plate can be inserted under the thigh muscles. The screws can be inserted into the proximal end of the plate through the existing lateral plate osteosynthesis approach. It is important to make sure that the plates do not end at the same level proximally to avoid a stress raiser (21). When there is a comminuted periprosthetic fracture, the exact anatomical reduction of the individual fragments is not recommended. Fracture-bridging biological osteosynthesis should restore the original axis, length, and rotation of the involved femur. It is advisable to use a lateral locking plate osteosynthesis with an additional medial helix plate to provide more stability. Any existing implants in the area of the proximal femur should be taken into account when selecting the osteosynthesis. An appropriately large implant-free bone section between proximal and distal implants has to be kept in mind. Biomechanically, it is better if the implants overlap on a defined area of bone. Kissing implants, in which proximally and distally positioned implants such as intramedullary nails, prosthetic stems, or plates only touch but do not overlap, should be avoided to prevent stress concentration in the junction zone that occurs under load (22). Bone grafts are used to support the medial column and prevent loss of reduction before the introduction of locking plates (23). Bone grafts are sometimes used in the revision of failed osteosyntheses of periprosthetic fractures (3,13,17). In type 3 fractures, the prosthesis is loose. It has to be replaced during the revision surgery. If a loosening of the implant cannot be safely ruled out before the operative revision, it is essential that an appropriate revision system is available in the treating institution. Due to deficient bone stock, the re-insertion of a surface replacement prosthesis is usually no longer possible. Stemmed revision prostheses are used in such cases. Depending on the bone loss, these prostheses are fixed or supported in the remnant of the femur with augments and cones. The ligamentous apparatus of the knee joint is often affected by the fracture or revision procedure, therefore rotating hinge prostheses are used in this situation. In most cases, the tibial component has also been changed to a stemmed model for reasons of stability and compatibility. If the distal femur has a large bony defect, the distal femoral replacement arthroplasty can be done. Following this procedure full weight-bearing is possible immediately postoperatively. This is of benefit to older patients who are unable to postoperatively ambulate partial weight-bearing. In distal femoral replacement arthroplasty, the force is applied in the area of the diaphysisis and not in the area of the condyles. Stress risers in the area at the tip of the stem lead to frequent fractures. Besides the high implant cost, a further disadvantage is that the origins of the musculus gastrocnemius medialis and lateralis must be detached during the procedure. The implantation of such a modular mega prosthesis is done usually as a salvage procedure (24,25).
Helix plate
Due to the already existing implants in patients with periprosthetic fractures, it is sometimes difficult to achieve a sufficient number of corticales both proximally and distally. This problem can be solved by using the medially inserted helix plate. The postoperative period of partial weight-bearing is about 15 weeks on average. The fracture consolidates with subsequent full weight-bearing. The average knee flexion of 85°–90° can be obtained.
The application of an additional medial helix locking plate seems to be a successful procedure for complex periprosthetic fractures such as interprosthetic fracture, presence of proximal implants, osteoporosis, non-union, or refracture after initial osteosynthesis.
Patella
The incidence of patella fractures in patients with TKR is 1.19%. The majority of these periprosthetic fractures occur in patients with an inlaid patellar resurfacing. Risk factors for such fractures include extensive bone resection when preparing the patella with a remaining patella thickness of less than 15 mm, malalignment with subluxation of the patella, devascularization of the patella through lateral release, incorrect positioning of components, use of cementless implants or implants with a single central fixation peg.
Radiological diagnostics is of particular importance since the incorrect positioning of the components plays a major role in the occurrence of periprosthetic patella fractures. To analyze the rotation of the components, a rotational CT of the entire affected leg is needed. If there is significant malrotation of the tibial or femoral component, new implantation with correct alignment has to be performed as part of the fracture management.
Periprosthetic patella fractures are usually not caused by direct trauma (5,26). The Ortiguera and Berry classification is suitable for decision-making in patella fractures around patellar resurfacing (27). This classification takes into consideration the condition of the extensor mechanism, bone stock, and implant fixation. In type 1 fractures, the extensor mechanism is intact and the patellar resurfacing is well-fixed. Type 1 fractures can be treated conservatively with initial immobilization in a cast and then gradual knee mobilization (28). In type 2 fractures there is interruption of the extensor apparatus with or without loosening of the patellar component. For such fractures, reconstruction of the extensor mechanism with osteosynthesis of the patella is needed. If the implant is loose, it has to be replaced. In type 3 fractures, the patella component is loosened but the extensor apparatus is intact. There are 2 subtypes of type 3 fractures. They can be distinguished depending on the bone stock after the removal of the inserted patella component. In subtype A the bone stock is good. A remaining patella thickness of 8 to 12 mm is considered sufficient to replace it with a conventional cemented polyethylene surface (29). A biconvex patella component can be implanted to compensate for the bony deficit if the thickness is less. For this purpose, the remaining bone stock must have a continuous bony margin (30). In patients with pronounced bone loss with poor support of the patella implant, a trabecular metal prosthesis can be used to fill the bony defect and establish good bony contact. The polyethylene component can then be fixed to this metal back with cement (31). In subtype B, the remaining bone stock is so deficient that no new patellar resurfacing can be done. After the removal of the patella component, patelloplasty can be done to shape the remaining patella. A Gullwing osteotomy involves incomplete vertical osteotomy of the patella in its center. Then the lateral and medial halves are arranged in a V-shape to each other to create a central ridge that can enter the groove of the femoral component to improve patella tracking and thus extensor function (32). Another available option is patella augmentation using autologous bone grafting in a retropatellar tissue flap (33). The ultimate option is a patellectomy which can produce significant impairment of the stability and biomechanics of the extensor apparatus (5).
Tibia
In patients with TKR periprosthetic fractures of the proximal tibia rarely occur. They can be classified according to the Felix classification depending on their localization, stability of the tibial component, and the moment of their occurrence. Type 1 fractures are located far proximally. They affect only a part of the proximal tibia and extend to the cranial interface of the tibial component. In type 2 fractures, the fracture line runs along the shaft of the tibial component, and in type 3 fractures the fracture line runs below it. The periprosthetic fractures that affect the insertion area of the knee joint extensor apparatus are classified as type 4 fractures. In subtype A there is a stable bony fixation of the tibial plateau. In subtype B the tibial implant is loose. Subtypes A and B imply the postoperative occurrence or detection of the fracture. Subtype C describes an intraoperative fracture (34). Risk factors for the occurrence of a periprosthetic fracture of the proximal tibia include the use of non-cemented implants, malposition of the tibial component, prior high tibial osteotomy, forced compaction of the cancellous bone and impaction of the tibial component during implantation, prior loosening of the components, and cortical impingement in long-stem prostheses. The assessment of the prosthesis fixation is important in the choice of the treatment concept. In the case of a loosened tibial component according to subtype B, it is mandatory to change this component, because a single osteosynthesis alone does not provide sufficient stability for the bony fixation of the prosthesis and it consequently leads to a dislocation of the component (3). During the revision of the tibial component, larger bone defects that affect the support of the prosthesis are filled with augments or cones. The treatment of periprosthetic tibial fractures of subtype A follows the usual principles of traumatology. Surgical treatment involves open reduction with plate or screw fixation. Depending on their level intraoperative fractures of subtype C can also be treated with osteosynthesis. In patients with type 3C fractures, the fracture can be bridged by the insertion of a longer prosthetic stem and stabilizing with plate osteosynthesis. Haller et al. described a technique of antegrade intramedullary nail osteosynthesis for diaphyseal type 3 fractures (35). Type 1A and type 1C fractures with small fragments that are not significantly displaced can be treated conservatively with immobilization in a femoral cast (15,36). Type 4 fractures involve the tibial tuberosity. Depending on the size of the fragment, screw or plate osteosynthesis can be carried out (3). Since the extensor apparatus of the knee joint is affected in this type of fracture, the flexion of the affected knee joint should initially be limited utilizing an orthosis and then gradually released to minimize tension on the extensor mechanism. Active extension of the knee against resistance should be avoided for the time of bone healing 6 weeks postoperatively. When planning osteosynthesis for proximal tibial fractures, it should be kept in mind that less soft tissue coverage can be achieved compared to the distal femur. Hence, risks such as postoperative wound healing or infections are more common.
Conclusion
The treatment goal should be a well-aligned and mobile knee joint combined with a pain-free, unassisted, fully ambulatory patient.
The decision regarding treatment options should be a team decision, involving an orthopedic surgeon, an anesthesiologist, an internal medicine specialist, and the patient. In patients with stable fractures and those who are not fit for surgery due to medical comorbidities, conservative non-surgical methods can be used that yield acceptable results. In patients who have stable or unstable fractures, but possess good bone stock and stable prosthesis, the choices include both intramedullary nailing and locking plate. External fixation is a method that allows early ambulation with the preservation of soft tissue while showing good results. Fractures with unstable prosthetic components but good bone stock should be treated with revision surgery. Fractures with poor bone stock and unstable prosthesis should be treated with endoprosthesis.
References
Kurtz S., Ong K., Lau E., Mowat F., Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780–785. doi: 10.2106/JBJS.F.00222.
Meek R.M.D., Norwood T., Smith R., Brenkel I.J., Howie C.R. The risk of peri-prosthetic fracture after primary and revision total hip and knee replacement. J Bone Joint Surg Br. 2011;93(1):96–101. doi: 10.1302/0301-620X.93B1.25087.
Ruchholtz S., Tomás J., Gebhard F., Larsen M.S. Periprosthetic fractures around the knee—the best way of treatment. Eur Orthop Traumatol. 2012;4(2):93–102. doi: 10.1007/s12570-012-0130-x.
Kim K.-I., Egol K.A., Hozack W.J., Parvizi J. Periprosthetic fractures after total knee arthroplasties. Clin Orthop Relat Res. 2006;446:167–175. doi: 10.1097/01.blo.0000214417.29335.19.
Chalidis B.E., Tsiridis E., Tragas A.A., Stavrou Z., Giannoudis P.V. Management of periprosthetic patellar fractures. Injury. 2007;38(6):714–724. doi: 10.1016/j.injury.2007.02.054.
Mittlmeier T., Beck M., Bosch U., Wichelhaus A. Periprosthetic knee fractures. Orthopä. 2015;45(1):54–64. doi: 10.1007/s00132-015-3205-x.
Fritz J., Lurie B., Potter H.G. MR imaging of knee arthroplasty implants. Radiographics. 2015;35(5):1483–1501. doi: 10.1148/rg.2015140216.
Su E.T., DeWal H., Di Cesare P.E. Periprosthetic femoral fractures above total knee replacements. J Am Acad Orthop Surg. 2004;12(1):12–20. doi: 10.5435/00124635-200401000-00003.
Fulkerson E., Tejwani N., Stuchin S., Egol K. Management of periprosthetic femur fractures with a first generation locking plate. Injury. 2007;38(8):965–972. doi: 10.1016/j.injury.2007.02.026.
Cain P.R., Rubash H.E., Wissinger H.A., McClain E.J. Periprosthetic femoral fractures following total knee arthroplasty. Clin Orthop Relat Res. 1986;208:205–214.
Merkel K.D., Johnson E.W. Supracondylar fracture of the femur after total knee arthroplasty. J Bone Joint Surg Am. 1986;68(1):29–43.
Herrera D.A., Kregor P.J., Cole P.A., Levy B.A., Jönsson A., Zlowodzki M. Treatment of acute distal femur fractures above a total knee arthroplasty: systematic review of 415 cases (1981–2006) Acta Orthop. 2009;79(1):22–27. doi: 10.1080/17453670710014716.
Wood G.C.A., Naudie D.R., McAuley J., McCalden R.W. Locking compression plates for the treatment of periprosthetic femoral fractures around well-fixed total hip and knee implants. J Arthroplasty. 2011;26(6):886–892. doi: 10.1016/j.arth.2010.07.002.
Graham S.M., Moazen M., Leonidou A., Tsiridis E. Locking plate fixation for Vancouver B1 periprosthetic femoral fractures: a critical analysis of 135 cases. J Orthop Sci. 2013;18(3):426–436. doi: 10.1007/s00776-013-0359-4.
Platzer P., Schuster R., Aldrian S. Management and outcome of periprosthetic fractures after total knee arthroplasty. J Trauma. 2010;68(6):1464–1470. doi: 10.1097/TA.0b013e3181d53f81.
Mittlmeier T., Beck M. Retrograde Verriegelungsmarknagelung bei periprothetischer distaler Femurfraktur nach kondylärem Kniegelenkersatz. Unfallchirurg. 2005;108(6):497–502. doi: 10.1007/s00113-005-0956-6.
Hagel A., Siekmann H., Delank K.-S. Periprosthetic femoral fracture. Dtsch Arztebl Int. 2014:1–7. doi: 10.3238/arztebl.2014.0658.
Rorabeck C.H., Taylor J.W. Classification of periprosthetic fractures complicating total knee arthroplasty. Orthop Clin N Am. 1999;30(2):209–214. doi: 10.1016/s0030-5898(05)70075-4.
Holzman M.A., Hanus B.D., Munz J.W., O'Connor D.P., Brinker M.R. Addition of a medial locking plate to an in situ lateral locking plate results in healing of distal femoral nonunions. Clin Orthop Relat Res. 2016;474(6):1498–1505. doi: 10.1007/s11999-016-4709-3.
Steinberg E.L., Elis J., Steinberg Y., Salai M., Ben-Tov T. A double-plating approach to distal femur fracture: a clinical study. Injury. 2017;48(10):2260–2265. doi: 10.1016/j.injury.2017.07.025.
Perren S.M., Regazzoni P., Fernandez A.A.D. Biomechanical and biological aspects of defect treatment in fractures using helical plates. Acta Chir Orthop Traumatol Cech. 2014;81(4):267–271.
Harris T., Ruth J.T., Szivek J., Haywood B. The effect of implant overlap on the mechanical properties of the femur. J Trauma. 2003;54(5):930–935. doi: 10.1097/01.TA.0000060999.54287.39.
Wang J.-W., Wang C.-J. Supracondylar fractures of the femur above total knee arthroplasties with cortical allograft struts. J Arthroplasty. 2002;17(3):365–372. doi: 10.1054/arth.2002.31077.
Berend K.R., Lombardi A.V., Jr. Distal femoral replacement in nontumor cases with severe bone loss and instability. Clin Orthop Relat Res. 2008;467(2):485–492. doi: 10.1007/s11999-008-0329-x.
Jassim S.S., McNamara I., Hopgood P. Distal femoral replacement in periprosthetic fracture around total knee arthroplasty. Injury. 2014;45(3):550–553. doi: 10.1016/j.injury.2013.10.032.
Mittlmeier T., Stöckle U., Perka C., Schaser K.D. Periprosthetic fractures after total knee joint arthroplasty. Unfallchirurg. 2005;108(6):481–496. doi: 10.1007/s00113-005-0955-7.
Ortiguera C.J., Berry D.J. Patellar fracture after total knee arthroplasty. J Bone Joint Surg Am. 2002;84(4):532–540. doi: 10.2106/00004623-200204000-00004.
Benkovich V., Klassov Y., Mazilis B., Bloom S. Periprosthetic fractures of the knee: a comprehensive review. Eur J Orthop Surg Traumatol. 2019;30(3):387–399. doi: 10.1007/s00590-019-02582-5.
Maheshwari A.V., Tsailas P.G., Ranawat A.S., Ranawat C.S. How to address the patella in revision total knee arthroplasty. Knee. 2009;16(2):92–97. doi: 10.1016/j.knee.2008.08.003.
Erak S., Bourne R.B., MacDonald S.J., McCalden R.W., Rorabeck C.H. The cemented inset biconvex patella in revision knee arthroplasty. Knee. 2009;16(3):211–215. doi: 10.1016/j.knee.2008.11.002.
Ries M.D., Cabalo A., Bozic K.J., Anderson M. Porous tantalum patellar augmentation: the importance of residual bone stock. Clin Orthop Relat Res. 2006;452:166–170. doi: 10.1097/01.blo.0000229359.27491.9f.
Gililland J.M., Swann P., Pelt C.E., Erickson J., Hamad N., Peters C.L. What is the role for patelloplasty with gullwing osteotomy in revision TKA? Clin Orthop Relat Res. 2015;474(1):101–106. doi: 10.1007/s11999-015-4363-1.
Hanssen A.D. Bone-grafting for severe patellar bone loss during revision knee arthroplasty. J Bone Joint Surg Am. 2001;83(2):171–176. doi: 10.2106/00004623-200102000-00003.
Felix N.A., Stuart M.J., Hanssen A.D. Periprosthetic fractures of the tibia associated with total knee arthroplasty. Clin Orthop Relat Res. 1997;(345):113–124.
Haller J.M., Kubiak E.N., Spiguel A., Gardner M.J., Horwitz D.S. Intramedullary nailing of tibial shaft fractures distal to total knee arthroplasty. J Orthop Trauma. 2014;28(12):e296–e300. doi: 10.1097/BOT.0000000000000096.
Born C.T., Gil J.A., Johnson J.P. Periprosthetic tibial fractures. J Am Acad Orthop Surg. 2018;26(8):e167–e172. doi: 10.5435/JAAOS-D-16-00387.
No comments:
Post a Comment