Terrible triad injury of the elbow
Dr. KS Dhillon
Introduction
The terrible triad injury of the elbow was originally described by Hotchkiss in 1996. It constitutes a highly unstable form of fracture-dislocation of the elbow. It consists of elbow dislocation with concomitant radial head or neck and coronoid process fractures [1,2,3].
This injury pattern is designated as terrible because of historically poor outcomes and high complication rates. The elbow is well known as one of the most stable joints of the body. The complex anatomical structure and higher functional requirements make treating the elbow injuries more difficult [4].
Owing to its complex anatomical structure, even isolated elbow dislocations without bony fragmentation involve substantial soft tissue injury with capsular and ligamentous disruption. In complex elbow dislocations, there
are fractures of one or more major bony stabilizers. Fractures can involve the radial head, coronoid process, or olecranon. These fractures can destabilize the dislocation and nearly always need operative intervention to restore functional anatomic alignment and joint stability [5].
Controversies remain regarding the appropriate treatment algorithm for these injuries despite clinical and operative advancements and an increased understanding of pathoanatomy and elbow biomechanics. Successful evaluation and treatment require detailed knowledge of the elbow anatomy, functional importance, and its contribution to elbow stability [5].
Anatomy
The elbow joint (fig 1) consists of three sub-joints, namely the humeroradial, humeroulnar, and superior radioulnar joints. The joints are enveloped by a common joint capsule. The humerus, radius, ulna, and related capsules, and ligaments make up these sub-joints. These joints allow elbow flexion and extension, and forearm pronation and supination. The coronoid process is a triangular-shaped protrusion at the proximal ulna and it plays a major role in keeping the elbow stable. Apart from bony structures, several ligaments also contribute to elbow stability. These include the medial collateral ligament complex (MCLC) and the lateral collateral ligament complex (LCLC). The MCLC is composed of three small ligaments namely the anterior medial collateral ligament, the posterior medial collateral ligament, and Cooper's ligament. The LCLC is made up of four small ligaments: the lateral ulnar collateral ligament, the lateral radial collateral ligament, the annular ligament, and the accessory lateral ligament. The stability of the elbow largely depends on the functions of the radial head, coronoid process of the ulna, LCLC, and the anterior medial collateral ligament.
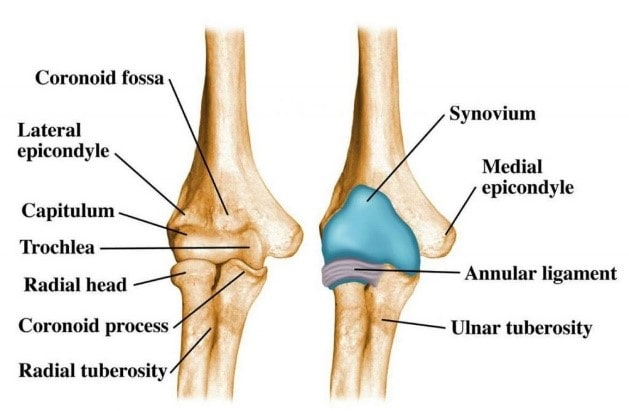
Fig 1- elbow joint
Etiology
About 60% of complex dislocations are caused by a fall from standing height [6]. Considerable force is required to sustain a complex dislocation. Falling on an extended arm that precludes valgus, axial, and posterolateral rotational forces, producing a posterolateral dislocation, is often the mechanism of insult.[1]
Fracture dislocations of the elbow tend to occur in distinct patterns depending on the mechanism of injury. Elbow extension with forearm supination and added valgus stress puts the most strain on the ulnohumeral joint, radial head, and MCL respectively. This causes a posterolateral rotational instability pattern of fracture-dislocation which includes posterior dislocation with a radial head fracture and the terrible triad injury with an added coronoid fracture. An axial load to the elbow in extension and a varus stress will cause compression injury to the medial side of the elbow leading to coronoid fractures, and tension forces acting laterally causing LCL rupture [7]. With the elbow in more flexion, this pattern can also cause a fracture of the olecranon. The outcome from this mechanism of injury is termed as varus posteromedial rotational instability. A direct blow to the posterior aspect of the flexed elbow can cause an anterior dislocation with an olecranon fracture. A hyperextension injury can also cause anterior dislocation with an olecranon fracture.
Epidemiology
Radial head fractures constitute between 20% to 30% of all adult elbow fractures [1]. Eighty-five percent of radial head fractures occur between the ages of 30 to 60 years. The mean occurrence is at age 45 years [8].
Coronoid fractures constitute 10% to 15% of elbow injuries. The elbow is the second most commonly dislocated joint, although it is one of the most stable joints in the body. About 20% of dislocations are associated with a fracture [6,9,10].
Pathophysiology
The elbow is made up of three sub-joints namely the humeroradial, humeroulnar, and superior radioulnar joints. The subjoints are made up of the humerus, radius, ulna, and related capsuloligamentous structures [11,12].
The radial head is an important restraint to posterolateral rotatory instability and it also acts as a secondary valgus stabilizer. In a normal elbow, the radial radiocapitellar articulation contributes minimally to valgus stability. However, in the event of MCL or coronoid injury, the radial head acts as the primary stabilizer to valgus stresses. It also prevents elbow subluxation[10]. Radial head fractures can be associated with episodic elbow instability, mechanical block to elbow motion, and injury to the distal radioulnar joint and/or the interosseous membrane (Essex-Lopresti) [13].
The coronoid process of the ulna provides ulnohumeral stability anteriorly and a varus buttress while resisting posterior subluxation [11].
The lateral collateral ligament (LCL) and medial collateral ligament (MCL) are the main capsuloligamentous stabilizers of the elbow. The MCL is the main stabilizer of valgus movements. It consists of the anterior bundle, posterior bundle, and transverse ligament. The robust anterior bundle is most important for stability [11]. Cavaderic studies have shown that fracture dislocations of the elbow are most likely to occur between 15 degrees of extension and 30 degrees of flexion, where the MCL is the least effective [14]. The lateral collateral ligament is the primary restraint to posterolateral rotatory instability. It contains four components namely the lateral ulnar collateral ligament, radial collateral ligament, annular ligament, and accessory (posterior) collateral ligament. The lateral ulnar collateral ligament is most important for stability [11].
The humeroulnar joint is the primary contributor to elbow stability, with its highly constrained articulation. The anteromedial facet resists varus movements and the muscles crossing the elbow joint contribute dynamically. The osseous and ligamentous structures afford static stability.
In the terrible triad, the structures of the elbow fail from lateral to medial as the forearm supinates and is loaded. There is disruption of the lateral collateral ligament first, then the anterior capsule, and finally the medial collateral ligament [6]. The pattern of disruption from lateral to anterior/posterior and then medial is commonly referred to as the Horri circle [15].
History and Physical Examination
The initial evaluation should proceed according to the Advanced Trauma Life Support (ATLS) protocol. Concomitant fractures, dislocations, and injuries throughout the ipsilateral extremity have to be excluded.
Distal radioulnar joint (DRUJ) tenderness may represent an interosseous ligament disruption and there may be concurrent Essex-Lopresti injury [13].
Fracture-dislocations of the elbow will present with swelling, pain, and deformity. There will be limitation of movements of the elbow [6][4].
A thorough neurovascular examination should be carried out. The ulnar nerve is most vulnerable to injury. Brachial artery injury, although rare, can occur and lead to ischemia and compartment syndrome [16].
Elbow stability is tested by doing a posterolateral drawer and posterolateral pivot shift tests, and varus/valgus instability stress testing. The DRUJ examination is done by palpating over the wrist for tenderness and translation of more than 50% in the sagittal plane. The interosseous membrane is palpated for tenderness. A radial pull test is done at the time of surgery and if there is more than 3 mm translation, there should be a concern for longitudinal forearm instability (Essex-Lopresti) [13]. When the patient presents in a delayed or recurrent fashion, the examiner should assess elbow flexion/extension, forearm rotation, and nerve function.
Evaluation
Anteroposterior and lateral radiographs are done for diagnosis. Additional shoulder, wrist, and hand imaging is done if the injury is suspected in other joints of the ipsilateral limb. Radiographs will help to evaluate the concentricity of humeroulnar and radiocapitellar joints. Lateral films will help in detecting coronoid fractures. Most injuries can be diagnosed with plain radiographs. A computed tomography (CT) scan is always obtained for patients with the terrible triad to identify fracture patterns, comminution, and displacement, that may not be evident on plain radiographs. Reconstructed CT scans are useful to better evaluate the injury pattern and assist with preoperative planning [17].
The CT scan will show coronoid, radial head, or olecranon injuries missed on initial radiographs. Fluoroscopic imaging under anesthesia is beneficial for intraoperative decision-making. When radiographs cannot be done after the injury in select patient populations, performing an examination under anesthesia while taking the elbow through gentle ROM is useful.
Nonstandard views may need to be obtained for joints that are stiff and the position cannot be changed to further assess the integrity and alignment of articulating surfaces.
There are several classifications available that can assist in further diagnostics. These are the Mason, Regan and Morrey, and O’Driscoll Classifications [18].
The Mason Classification for Radial Head Fractures:
Type I radial head fractures are either nondisplaced or minimally displaced (less than 2 mm), with no mechanical block to rotation.
Type II are displaced (more than 2 mm) or angulated fractures, with possible mechanical block to forearm rotation.
Type III have fracture comminution and displacement with confirmed mechanical block to motion.
Type IV radial head fractures are associated with elbow dislocation[11].
The Regan and Morrey Classification system identifies three types of coronoid fractures:
Type I involves the coronoid tip
Type II describes a fracture involving 50% or less of coronoid height
Type III is determined by a fracture of greater than 50% of coronoid height [6,11].
The O’Driscoll Classification system subdivides coronoid injuries based on location and the number of coronoid fragments. It recognizes that anteromedial facet fractures are caused by varus posteromedial rotatory forces [19].
Treatment
The aim of treatment is to reestablish enough stability to permit early movements of the elbow [9,20,21]. Anatomic alignment of osseous structures is re-established. This is followed by restoration of the radial head and radiocapitellar contact. Ligaments are repaired if necessary.
If the elbow is sufficiently stable to allow early mobilization, non-operative management with immobilization in 90 degrees of flexion for 7 to 10 days is indicated. Non-operative treatment is also indicated if the coronoid fracture is small, the radial head fracture does not need surgery, and the humeroulnar and radiocapitellar joints have been anatomically reduced. A progressive range of movement exercises is routinely instituted following one week of immobilization. Strengthening protocols are begun after six weeks.
An unstable radial head fracture and type III coronoid fracture, with associated elbow dislocation, is an indication for operative intervention. Open reduction internal fixation (ORIF) of the radial head, LCL reconstruction, and coronoid ORIF, with possible MCL reconstruction is carried out. In some situations, a radial head replacement may be necessary. If the instability persists after addressing the radial head and LCL complex, the next step is to proceed with operative MCL reconstruction.
Isolated dislocations of the elbow are treated by immediate closed reduction. The reduction can be done in the emergency department under sedation. Successful reduction is accompanied by a clunking sound. The elbow should then be tested for stability by moving the elbow through a range of movements. Postreduction X-rays are done to confirm reduction. The elbow is then splinted in 90 degrees of flexion. Splinting should not proceed beyond three weeks.
When surgery is indicated for radial head fractures, open reduction internal fixation (ORIF) is usually done. Radial head resection in fracture-dislocations may lead to Essex-Lopresti instability and arthrosis. Every effort should be made to maintain radial head integrity [10].
Open reduction and internal fixation is ideally carried out for radial head fractures when the fracture is non-comminuted and involves more than 40% of the articular surface and demonstrates bony continuity between the radial head and neck. Intra-osseous screws, compression screws, retrograde pinning, or anatomic plates can be utilized for fixation. When a plate is used it must be positioned posterolaterally in the safe zone, with the forearm in neutral, to minimize the risk of injuring the posterior interosseous nerve. Radial head arthroplasty is done for patients with a comminuted/displaced fracture of more than three fragments.
For radial head arthroplasty appropriately-sized implants must be used. A prosthetic head that is too small provides a very narrow area of contact which causes LCL laxity. If the head is too large it leads to poor congruence and excessive LCL tensioning, leading to postoperative stiffness. Patients undergoing arthroplasty with radial head replacement have demonstrated fewer postoperative complications, with significantly better ROM, than radial head repair [20]. When there is no coronoid fracture, a radial head fracture with elbow dislocation can be treated non-operatively.
Type 3 coronoid fractures should be treated operatively [10]. In type 1 and type 2 fractures, there should be radial head conservation, elbow stability, and bony column congruence following soft tissue reconstruction. The coronoid can be repaired with sutures, anchors, screws, or the “suture lasso” technique. Open reduction internal fixation is the most common treatment for terrible triad injuries [6,10]. Coronoid fractures can be fixed via ORIF through the radial head defect laterally.
When a medial approach is used, the median antebrachial cutaneous nerve should be preserved. The coronoid fracture can be exposed between the two heads of the flexor carpi ulnaris. The ulnar nerve should always be visualized and protected. The lateral approach provides better access to the coronoid process. Postoperatively, active and active-assist ROM therapy is begun after 10-14 days.
The LCL is repaired with the forearm in pronation if the MCL is intact. If MCL is injured, LCL is repaired with the forearm in supination. Postoperatively, it is important to avoid excessive shoulder abduction because that places undue stress on the LCL repair. Stability and adequate elbow function could be operatively restored without repairing the MCL. However, in cases where the elbow remains unstable after fracture fixation and lateral soft tissue (LCL) repair, especially in extension beyond 30 degrees, the MCL should be repaired [10,11,21].
Terrible triad injuries following high-energy insults are often accompanied by severe soft tissue injuries. This further prolongs the time to operative treatment, as soft tissue requirements for successful surgical outcomes are met in the interim. Several studies have documented that longer delays to surgery from injury produces postoperative elbow stiffness. Zhou et al [3] found that prognostication is optimized when surgical treatment is done between 24 hours and 14 days after injury.
Lindenhovius et al [4] demonstrated a better range of motion in patients who underwent surgery within two weeks after the injury [4]. Wiigger et al. found that every 24-hour delay in surgery following initial injury more than doubles the risk of postoperative elbow stiffness [4].
Prognosis
Terrible triad injury patterns have historically poor outcomes due to persistent instability, stiffness, and arthrosis. A high index of suspicion is needed to expeditiously proceed through a detailed extremity examination, and appropriate imaging studies to make a correct diagnosis and proceed with early proper treatment [13].
Complications
Complications following elbow fracture-dislocation include synostosis, arthrofibrosis, heterotopic ossification (HO), infection, recurrent instability, post-traumatic arthritis, stiffness, nonunion, ulnar neuropathy, loosening of implant, and symptomatic hardware. Surgery to treat terrible triad injuries is associated with a high risk of complications, with up to a 54.5% reoperation rate, averaging between 22% to 30% [6,21,22].
Anatomic reduction of intraarticular fractures is necessary to prevent arthritic changes. A slight loss of extension can be expected. About 5% to 15% of patients with elbow fractures will experience stiffness following surgery [4]. Arthritis is common after high-energy trauma. It is likely a sequela of initial chondral impact and the degree of recurrent elbow instability.
Some loss of motion after elbow fracture-dislocation can be expected. Patients usually lose more extension than flexion. The amount of stiffness increases with the energy of the initial injury. Heterotopic bone formation and delay of motion after repair also increase the amount of stiffness.
Post-traumatic calcium deposition in the collateral ligaments and capsule is relatively common. Some reports document just under a 20% occurrence rate. Heterotopic ossification (HO) has occurred in up to 43% of operatively treated fracture dislocations [23,24].
Heterotopic ossification can cause near-complete ankylosis of the elbow. This can be seen on radiographic imaging 3 to 4 weeks after injury. The frequency and severity of HO are associated with the severity of the injury, the extent of soft tissue damage, length of immobilization, neurological injury, infection, delay to surgery, and the presence of associated burns [24]. Heterotopic ossification most often occurs either anteriorly, between the capsule and brachialis, or posteriorly, between the capsule and triceps.
Distraction forces across the fracture secondary to flexion or active extension can lead to nonunion. Internal fixation failure is most common following radial neck fracture repairs secondary to its inherently poor vascularity. Recurrent instability rates are low. The most common cause is failure to recognize or treat fracture(s) or ligamentous injury. Recurrent instability is more common following type I or II coronoid fractures.
Postoperative and Rehabilitation Care
Postoperative splinting is done for up to 10 days, depending on the stability achieved and concurrent injuries. The splint may be placed in flexion with the forearm in pronation to provide stability against posterior subluxation. When both MCL and LCL are repaired, the splint is positioned in flexion and neutral rotation. Some patients can start ROM exercises on the first postoperative day, with a majority beginning active ROM within 48 hours. Forearm rotation is usually allowed. Shoulder and wrist exercises are performed without restrictions. Extension within the terminal 30 degrees of motion is avoided for four weeks.
The terrible triad of elbow injuries is difficult to treat. Despite optimal treatment and compliance with postoperative rehabilitation, rarely is it possible to achieve a full range of motion. Gomide et al [10] showed a mean flexion-extension range of 113 degrees and average flexion contracture of 24 degrees following surgery for terrible triad injuries of the elbow.
Conclusion
The terrible triad injury of the elbow is the most complex pattern of all dislocations. It combines ligament damage with radial head and coronoid process fractures. Complete dislocations of the elbow joint should be considered as a terrible triad injury unless proven otherwise. The lack of knowledge of this clinical pattern of injury might be detrimental to elbow function. CT scan assessment should be carried out after the dislocation has been reduced for proper investigation of bony lesions.
The principle objective of surgical management is to restore the bony stabilizing structures i.e. the radial head and coronoid process and radial collateral ligament reconstruction. Isolated radial head resection should be avoided since it appears as a bad prognosis factor for short and long-term outcome. Arthroplasty is advised if radial head fracture cannot be managed with osteosynthesis.
A medial surgical approach is recommended in patients with persistent posterolateral instability following radial collateral ligament reconstruction or when fixation of a large coronoid process fragment is necessary. External fixation is advocated when there is persistent instability following the reconstruction of bony and ligamentous structures. It provides joint stability and protects the reconstruction.
References
Galbiatti JA, Cardoso FL, Ferro JAS, Godoy RCG, Belluci SOB, Palacio EP. Terrible triad of the elbow: evaluation of surgical treatment. Rev Bras Ortop. 2018 Jul-Aug;53(4):460-466.
Ikemoto RY, Murachovsky J, Bueno RS, Nascimento LGP, Carmargo AB, Corrêa VE. TERRIBLE TRIAD OF THE ELBOW: FUNCTIONAL RESULTS OF SURGICAL TREATMENT. Acta Ortop Bras. 2017 Nov-Dec;25(6):283-286.
Zhou C, Lin J, Xu J, Lin R, Chen K, Sun S, Kong J, Shui X. Does Timing of Surgery Affect Treatment of the Terrible Triad of the Elbow? Med Sci Monit. 2018 Jul 09;24:4745-4752.
He X, Fen Q, Yang J, Lei Y, Heng L, Zhang K. Risk Factors of Elbow Stiffness After Open Reduction and Internal Fixation of the Terrible Triad of the Elbow Joint. Orthop Surg. 2021 Apr;13(2):530-536.
Ohl X, Siboni R. Surgical treatment of terrible triad of the elbow. Orthop Traumatol Surg Res. 2021 Feb;107(1S):102784.
Jones ADR, Jordan RW. Complex Elbow Dislocations and the "Terrible Triad" Injury. Open Orthop J. 2017;11:1394-1404.
Doornberg J.N., Ring D.C. Fracture of the anteromedial facet of the coronoid process. J. Bone Joint Surg. Am. 2006;88(10):2216–2224.
Kovar FM, Jaindl M, Thalhammer G, Rupert S, Platzer P, Endler G, Vielgut I, Kutscha-Lissberg F. Incidence and analysis of radial head and neck fractures. World J Orthop. 2013 Apr 18;4(2):80-4.
Papatheodorou LK, Rubright JH, Heim KA, Weiser RW, Sotereanos DG. Terrible triad injuries of the elbow: does the coronoid always need to be fixed? Clin Orthop Relat Res. 2014 Jul;472(7):2084-91.
Gomide LC, Campos Dde O, Ribeiro de Sá JM, Pamfílio de Sousa MR, do Carmo TC, Brandão Andrada F. TERRIBLE TRIAD OF THE ELBOW: EVALUATION OF SURGICAL TREATMENT. Rev Bras Ortop. 2011 Jul-Aug;46(4):374-9.
Xiao K, Zhang J, Li T, Dong YL, Weng XS. Anatomy, definition, and treatment of the "terrible triad of the elbow" and contemplation of the rationality of this designation. Orthop Surg. 2015 Feb;7(1):13-8.
Liman MNP, Avva U, Ashurst JV, Butarbutar JC. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Aug 8, 2022. Elbow Trauma.
Ramzi Z, Juanos Cabans J, Jennart H. Terrible triad of the elbow with an ipsilateral Essex-Lopresti injury: case report. J Surg Case Rep. 2020 Jun;2020(6):rjaa103.
Wake H., Hashizume H., Nishida K., Inoue H., Nagayama N. Biomechanical analysis of the mechanism of elbow fracture-dislocations by compression force. J. Orthop. Sci. 2004;9(1):44–50.
de Klerk HH, Oosterhoff JHF, Schoolmeesters B, Nieboer P, Eygendaal D, Jaarsma RL, IJpma FFA, van den Bekerom MPJ, Doornberg JN., Traumaplatform 3D Consortium. Recognition of the pattern of complex fractures of the elbow using 3D-printed models. Bone Joint J. 2023 Jan;105-B(1):56-63.
Gonzalez LJ, Shields CN, Leucht P, Konda SR, Egol KA. Fracture-Dislocations of the Elbow: A Comparison of Monteggia and Terrible Triad Fracture Patterns. Orthopedics. 2022 Dec 02;:1-6.
Ozdag Y, Luciani AM, Delma S, Baylor JL, Foster BK, Grandizio LC. Learning Curve Associated With Operative Treatment of Terrible Triad Elbow Fracture Dislocations. Cureus. 2022 Jul;14(7):e27156.
Lampaert S, Herregodts J, De Wilde L, Van Tongel A. Radial head fractures: a quantitative analysis. Acta Orthop Belg. 2022 Jun;88(2): 380-386.
Shukla DR, Fitzsimmons JS, An KN, O'Driscoll SW. Effect of radial head malunion on radiocapitellar stability. J Shoulder Elbow Surg. 2012 Jun;21(6):789-94.
Chen H, Shao Y, Li S. Replacement or repair of terrible triad of the elbow: A systematic review and meta-analysis. Medicine (Baltimore). 2019 Feb;98(6):e13054.
Kim BS, Kim DH, Byun SH, Cho CH. Does the Coronoid Always Need to Be Fixed in Terrible Triad Injuries of the Elbow? Mid-Term Postoperative Outcomes Following a Standardized Protocol. J Clin Med. 2020 Oct 29;9(11).
Chen HW, Liu GD, Wu LJ. Complications of treating terrible triad injury of the elbow: a systematic review. PLoS One. 2014;9(5): e97476.
Shukla DR, Pillai G, McAnany S, Hausman M, Parsons BO. Heterotopic ossification formation after fracture-dislocations of the elbow. J Shoulder Elbow Surg. 2015 Mar;24(3):333-8.
Tangtiphaiboontana J, Agel J, Beingessner D, Hébert-Davies J. Prolonged dislocation and delay to surgery are associated with higher rates of heterotopic ossification in operatively treated terrible triad injuries. JSES Int. 2020 Jun;4(2):238-241.
No comments:
Post a Comment