Avascular Necrosis of the Shoulder
Dr. KS Dhillon
Introduction
Osteonecrosis of the humeral head is a disorder that is characterized by bone death. It involves osteocytes and the bone marrow. The osteonecrosis can be traumatic or atraumatic. Osteonecrosis of the humeral head can result in the collapse of the humeral head and lead to joint destruction. The glenoid is not so constrained and it can accept greater deformity of the humeral head. The scapula can compensate for some of the glenohumeral motion loss.
Traumatic osteonecrosis occurs due to disruption of the blood supply caused by dislocation or fracture of the proximal humerus [1]. Atraumatic osteonecrosis is also due to abnormalities of humeral head blood flow. There are multiple etiologies for atraumatic osteonecrosis. Corticosteroid therapy is the most common cause. Atraumatic osteonecrosis can be multifocal or bilateral. Osteonecrosis is considered multifocal when three or more joints are involved. The femoral and humeral head are most often affected [2].
Disease prevention is very important. Those at risk must be identified. The preventive measures must be defined. Most cases can be treated without surgery. Identification of disease progression is very important to recognize and treat symptomatic disease in the early stages, thereby avoiding the need for arthroplasty.
Anatomy
The major blood supply to the humeral head comes from the ascending branch of the anterior humeral circumflex artery (fig 1). It enters the humeral head through the bicipital groove. The posterior humeral circumflex artery provides a small amount of collateral flow after piercing the rotator cuff attachments. Collateral blood flow around the proximal humerus is minimal. This puts the head at risk through trauma or other circulatory insults. Intraosseous blood supply to the head comes from the arcuate artery.
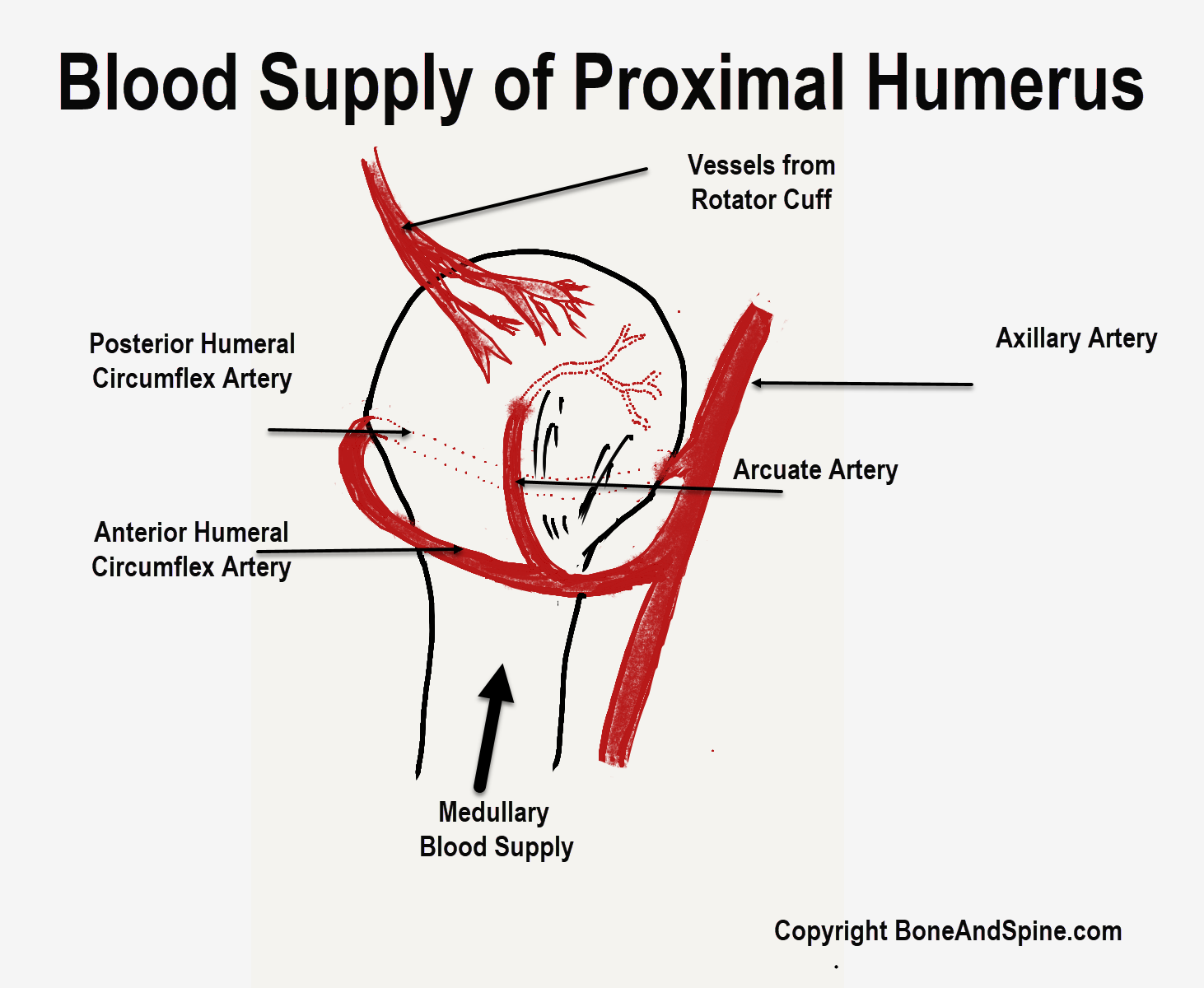
Fig 1.
Pathophysiology
The initiating insult to the humeral head differs depending on the cause. Mechanical disruption of the proximal humeral vasculature can occur due to trauma. For steroid-induced disease, there are several theories [3]. One of the theories is that increased intraosseous fat cell size results in increased intraosseous pressure and fat embolism. Alcohol consumption appears to work in the same way as steroids. Caisson disease or dysbarism causes congestion and ischemia leading to cell death via air bubbles. In patients with sickle cell disease, the sickled red blood cells cause infarcts in the subchondral bone.
After the initial insult, the pathogenesis of the disease is the same, regardless of the etiology. Death of the marrow and cells occurs. During the healing phase, bone resorption occurs to remove the necrotic tissue. During this phase of bone resorption, the bone is weakened. The forces across the subchondral plate of the weakened bone can lead to microfractures and subsequent collapse. With progressive deformity of the humeral head, the glenoid becomes involved with resultant arthritic changes.
Etiology
Traumatic shoulder osteonecrosis occurs due to disruption of the vascular supply of the humeral head due to a dislocation or a fracture. There are a growing number of publications that report shoulder osteonecrosis following arthroscopic rotator cuff surgery [4].
There are several causes of atraumatic osteonecrosis. Steroid use and alcohol abuse predominate. Other causes include dysbarism, Gaucher disease, hemoglobinopathies, coagulopathies, connective tissue disorders, and some idiopathic disorders [5,6]. Adults with sickle cell disease are at higher risk for shoulder osteonecrosis if they have hip osteonecrosis or if they have the S Beta or SC genotype [7].
Epidemiology
The incidence of osteonecrosis of the humeral head, particularly the atraumatic form, is not exactly known. It occurs less often than in the hip. The traumatic form has been reported in up to 34% of 3-part fractures and 90% of 4-part fractures. It occurs in nearly all patients with anatomical neck fractures.
The traumatic form of osteonecrosis can occur at any age in patients with 3-part, 4-part, or anatomic neck humeral fractures and/or dislocations. The atraumatic form usually occurs in patients aged between 20-60 years.
Prognosis
The forces transmitted through the shoulder joint are much less than those transmitted through the joints of the lower extremity. Therefore the symptoms can be mild, even in those with advanced disease. Many patients obtain good outcome with conservative treatment using analgesics and/or physical therapy for extended periods. Surgery is usually reserved for those with severe pain.
Clinical Presentation
The clinical presentation depends on the etiology. There is an insidious onset of pain often without a clear inciting event. Often the pain is poorly localized and can be severe. Night and rest pain are often present. The pain usually escalates with activity. In the early part of the disease, the range of motion (ROM) is preserved. Motion, however, causes pain. When there is subchondral collapse crepitation and locking can be present. When arthritis sets in the ROM decreases mechanically.
Laboratory Studies
There is no need for laboratory studies for the diagnosis of osteonecrosis. Inciting factors can be identified by certain tests such as:
Lipid profile to reveal if there is underlying hyperlipidemia
Sickle cell disease in African Americans
Thrombotic disorders - Protein S and protein C deficiencies, factor V Leiden disease
Imaging Studies
In most cases, radiographs help establish the diagnosis. The radiographic views include anteroposterior (AP) and axillary views. When radiographs are normal and there is clinical suspicion of humeral osteonecrosis, magnetic resonance imaging (MRI) is the diagnostic modality of choice. MRI has sensitivity and specificity greater than 98% [8]. The extent of humeral head necrosis on MRI can predict the possibility of future collapse of the humeral head [9].
Other imaging modalities include the following:
Tomography – Helpful in stage II disease to further define the lesion
Bone scan [8] – Can be useful when disease is suspected clinically but is not apparent on radiographs. It is not commonly used because of the high success rates of MRI
Other Tests
Additional studies that are sometimes carried out include:
Venography
Biopsy – Can be performed at the time of surgery (eg, core decompression)
Intraosseous pressure measurements
Histologic Pathology
In the initial phases of the disease, there is cell and marrow necrosis. In the reparative phase, the dead bone is removed and replaced by healthy bone. During this period, the bone is weak, and subchondral collapse can occur. Once collapse of the subchondral plate occurs, damage to the articular cartilage can occur leading to arthritic changes of the joint.
Staging
Humeral head osteonecrosis has been staged by Ficat and Arlet [10] :
Stage I - The humeral head is normal
Stage II - There are cystic and/or osteosclerotic lesions but the humeral head contour is normal
Stage III - There is subchondral collapse or crescent sign
Stage IV - There is narrowing of joint space and secondary osteoarthritic changes of the glenoid fossa and the humeral head, such as marginal osteophytes, cysts, and destruction of cartilage
Treatment
Treatment of humeral head osteonecrosis depends on the stage of the disease and the symptoms present. If the inciting factor has been recognized the important initial step is to eliminate it. Elimination of the inciting factor does not reverse the course of the disease process. Often treatment can be delayed or is not required because the shoulder is a non–weightbearing joint. In patients with severe pain and/or mechanical symptoms, conservative and surgical treatment options are available. There are no specific contraindications to treatment, other than those pertaining to high surgical risk situations. The presence of infection or severe systemic disease may preclude surgical intervention.
Medical Treatment
The first line of treatment is removal of the offending agent, if possible. Nonsurgical treatment is often more successful in cases of shoulder osteonecrosis than in hip osteonecrosis. This is because the shoulder is a non-weight-bearing joint. Nonsurgical treatment includes the use of medications for pain, physical therapy, and activity modification. Physical therapy includes modalities for pain control and range of motion (ROM) exercises with subsequent strengthening exercises. This is helpful in all stages, but particularly in stage I and stage II. Overhead activity and manual labor should be avoided.
Some studies show that treatment with alendronate can prevent a collapse of the femoral head caused by osteonecrosis. However, there is no research published regarding its effectiveness in treating osteonecrosis of the shoulder.
Surgical treatment
In patients with early disease core decompression is carried out. A central core of bone is removed or drilled from the humeral head into the necrotic zone [11]. The outcome of core decompression is good to excellent in up to 90% of cases of stage I and stage II disease [12,13]. Core decompression can also be successful in stage III disease, with a 30% failure rate. Failure occurs in all cases of stage IV. The procedure is only palliative [11]. An alternative technique of decompression utilizing multiple passes of a small-diameter (3-mm) drill has also been described [14].
Hernigou et al [15] carried out a prospective randomized clinical study of 50 patients with post-traumatic shoulder osteonecrosis. They compared the results of mesenchymal stem cell grafting of the humeral head versus core decompression. They found that after more than a decade of follow-up, the rate of collapse was significantly lower in the group treated with stem cells (11.55 vs 87.5%, P < 0.0001).
Limited experience with muscle pedicle grafting has shown no significant difference from core decompression alone [16]. Arthroscopic debridement of chondral lesions can be performed. Arthroscopy can help deal with mechanical symptoms.
Depending on the condition of the glenoid, hemiarthroplasty (HA) or total shoulder arthroplasty (TSA) can be done [17,18,19]. A 90% success rate has been reported for hemiarthroplasty and total shoulder arthroplasty in patients with advanced disease, with most patients regaining full ROM [17, 19]. Surface replacement arthroplasty can also be an option [20,21].
The decision to carry out a given surgical procedure is based on the preoperative staging. Core decompression, muscle pedicle grafting, and arthroscopy are indicated in cases before the collapse of the humeral head. These procedures are useful in stage I, stage II, and stage III disease.
Once irregularity of the joint surfaces occurs, arthroplasty is needed. In individuals with atraumatic osteonecrosis of the humeral head, both total shoulder arthroplasty and hemiarthroplasty can be expected to provide lasting pain relief and improved range of motion. Schoch et al [22] recommended that hemiarthroplasty be carried out in patients with atraumatic osteonecrosis of the humeral head who have preserved glenoid cartilage.
In a study by Schoch et al [23] that compared 37 HAs and 46 TSAs performed for post-traumatic osteonecrosis of the humeral head, HA provided improvements in range of motion but TSA provided superior pain relief with better patient-reported satisfaction.
Intraoperative details vary according to the procedure that is chosen.
Core decompression is performed as follows:
The patient is placed in the beach-chair position with the arm over the edge of the table. A small incision is made in the lateral deltoid. With image intensification, a K-wire is introduced into the necrotic lesion. A cannulated drill is used to take a core of bone.
If the drilling technique is used, instead of using a coring reamer, multiple passes are made into the lesion with a small-diameter drill (usually 3.2 mm) under image intensification.
Intraarticular debridement can be done by arthroscopy. Articular cartilage flaps can be debrided back to a stable rim. Any loose bodies present can be removed, and a selective capsular release can be performed if needed.
Hemiarthroplasty is done for moderate disease (stage III and IV disease). It involves the placement of a humeral head prosthesis, through a deltopectoral approach. The excised head is used as a sizer. A near perfect replacement of the articular surface can be achieved.
Total shoulder arthroplasty is done for advanced disease (stage IV disease). There are several prostheses available. The glenoid is resurfaced with an all-polyethylene component. Total shoulder arthroplasty is done in individuals with stage IV disease.
In surface replacement arthroplasty for stage III disease, the humeral head is resurfaced partially or completely with a metal component.
Postoperative Care
Immediate ROM exercises can be started in patients who have undergone core decompression and muscle pedicle grafting. There can be some limitations on ROM exercises in patients who had muscle pedicle grafting. Patients who had core decompression are started on immediate passive ROM exercises, with active ROM as tolerated. Once full ROM is achieved than strengthening exercises can be started.
In patients who have undergone hemiarthroplasty and shoulder arthroplasty, immediate passive ROM can be started. There should be limitation of external rotation to 45° for 6 weeks to allow for healing of the subscapularis. Active ROM can be started as tolerated. Strengthening exercises are usually initiated at 6 weeks post-surgery.
Complications
Surgical complications include infection and neurovascular injuries. These are, however, rare. When performing core decompression, care has to be taken to avoid the axillary nerve anteriorly. During core decompression penetration of the humeral head should be avoided.
With arthroplasty, potential complications include intraoperative fracture, dislocation, and prosthetic loosening. Fortunately, these problems are rare.
Conclusion
Osteonecrosis of the humeral head is a complex condition that is not fully understood. It most commonly occurs due to trauma or corticosteroid and alcohol use. It can also be associated with a variety of other risk factors such as blood dyscrasias and metabolic and coagulation disorders. Initial evaluation includes a thorough history and physical examination, as well as an assessment of plain radiographs of the shoulder and pelvis. Early-stage humeral osteonecrosis is best evaluated by MRI. CT scans can help identify subchondral fractures.
Treatment is usually nonsurgical. Surgery may be needed for patients with advanced disease.
References
Patel S, Colaco HB, Elvey ME, Lee MH. Post-traumatic osteonecrosis of the proximal humerus. Injury. 2015 Jun 19.
El Gamal TA, El-Bakoury A, Hawkins A, Ed AlTayeb Mussa M, Er Ahmed Sweed T, Eh Samir Ansara S. Bilateral Osteonecrosis of the Femoral and Humeral Heads after Short Term Corticosteroid Therapy. A Case Study. Ortop Traumatol Rehabil. 2016 Mar 23. 18 (2):187-190.
Cruess RL. Experience with steroid-induced avascular necrosis of the shoulder and etiologic considerations regarding osteonecrosis of the hip. Clin Orthop Relat Res. 1978 Jan-Feb. 86-93.
Keough N, Lorke DE. The humeral head: A review of the blood supply and possible link to osteonecrosis following rotator cuff repair. J Anat. 2021 Nov. 239 (5):973-982.
Cruess RL. Steroid-induced avascular necrosis of the head of the humerus. Natural history and management. J Bone Joint Surg Br. 1976 Aug. 58(3):313-7.
Cushner MA, Friedman RJ. Osteonecrosis of the Humeral Head. J Am Acad Orthop Surg. 1997 Nov. 5(6):339-346.
Hernigou P, Hernigou J, Scarlat M. Shoulder Osteonecrosis: Pathogenesis, Causes, Clinical Evaluation, Imaging, and Classification. Orthop Surg. 2020 Oct. 12 (5):1340-1349.
Mont MA, Ulrich SD, Seyler TM, Smith JM, Marker DR, McGrath MS, et al. Bone scanning of limited value for diagnosis of symptomatic oligofocal and multifocal osteonecrosis. J Rheumatol. 2008 Aug. 35(8):1629-34.
Sakai T, Sugano N, Nishii T, Hananouchi T, Yoshikawa H. Extent of osteonecrosis on MRI predicts humeral head collapse. Clin Orthop Relat Res. 2008 May. 466(5):1074-80.
Ficat RP, Arlet J. Necrosis of the femoral head. Hungerford DS. Ischemia and necrosis of bone. Baltimore, MD: Williams & Wilkins; 1980. 171-82.
Soohoo NF, Vyas S, Manunga J, Sharifi H, Kominski G, Lieberman JR. Cost-effectiveness analysis of core decompression. J Arthroplasty. 2006 Aug. 21(5):670-81.
LaPorte DM, Mont MA, Mohan V, Pierre-Jacques H, Jones LC, Hungerford DS. Osteonecrosis of the humeral head treated by core decompression. Clin Orthop Relat Res. 1998 Oct. 254-60.
Mont MA, Maar DC, Urquhart MW, Lennox D, Hungerford DS. Avascular necrosis of the humeral head treated by core decompression. A retrospective review. J Bone Joint Surg Br. 1993 Sep. 75(5):785-8.
Harreld KL, Marulanda GA, Ulrich SD, Marker DR, Seyler TM, Mont MA. Small-diameter percutaneous decompression for osteonecrosis of the shoulder. Am J Orthop (Belle Mead NJ). 2009 Jul. 38 (7):348-54.
Hernigou P, Hernigou J, Scarlat M. Mesenchymal stem cell therapy improved outcome of early post-traumatic shoulder osteonecrosis: a prospective randomized clinical study of fifty patients with over ten year follow-up. Int Orthop. 2021 Oct. 45 (10):2643-2652.
Kawamura K, Kawate K, Yajima H, Kobata Y, Takakura Y. Vascularized scapular grafting for treatment of osteonecrosis of the humeral head. J Reconstr Microsurg. 2008 Nov. 24(8):559-64.
Feeley BT, Fealy S, Dines DM, Warren RF, Craig EV. Hemiarthroplasty and total shoulder arthroplasty for avascular necrosis of the humeral head. J Shoulder Elbow Surg. 2008 Sep-Oct. 17(5):689-94.
Smith RG, Sperling JW, Cofield RH, Hattrup SJ, Schleck CD. Shoulder hemiarthroplasty for steroid-associated osteonecrosis. J Shoulder Elbow Surg. 2008 Sep-Oct. 17(5):685-8.
Tauber M, Karpik S, Matis N, Schwartz M, Resch H. Shoulder arthroplasty for traumatic avascular necrosis: predictors of outcome. Clin Orthop Relat Res. 2007 Dec. 465:208-14.
Raissp, Kasten P, Baumann F, Moser M, Rickert M, Loew M. Treatment of osteonecrosis of the humeral head with cementless surface replacement arthroplasty. JBJS(Am). Feb 2009. 91(2):340-9.
Uribe JW, Botto-van Bernden A. Partial humeral head resurfacing for osteonecrosis. J Shoulder Elbow Surg. Sept-Oct 2009. 18(5):711-6.
Schoch BS, Barlow JD, Schleck C, Cofield RH, Sperling JW. Shoulder arthroplasty for atraumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg. 2016 Feb. 25 (2):238-45.
Schoch BS, Barlow JD, Schleck C, Cofield RH, Sperling JW. Shoulder arthroplasty for post-traumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg. 2016 Mar. 25 (3):406-12.
No comments:
Post a Comment