Intersection Syndrome
Dr. KS Dhillon
Introduction
Intersection syndrome affects the first and second compartments of the dorsal wrist extensors. It occurs as a result of repetitive friction at the junction in which the tendons of the first dorsal compartment crosses over the second, creating tenosynovitis. It presents with pain just proximal and dorsal to the radial styloid, and 4 cm - 6 cm proximal to Lister's tubercle [1,2,3].
Most cases of intersection syndrome respond to conservative treatment. It consists of immobilization, activity modification, and pharmacologic intervention, followed by a program of supervised hand or occupational therapy. Refractory cases can be treated by surgery.
Etiology
Direct trauma to the second extensor compartment can cause intersection syndrome. It is usually brought on by activities that require repetitive wrist flexion and extension [4]. Rowers, weightlifters, horseback riders, and other athletes are particularly prone to this condition [5,6,7].
Repetitive movements at the wrist results in friction at the crossover junction of the 1st and 2nd dorsal compartments. The friction leads to an inflammatory response and subsequent tenosynovitis.
Pathophysiology
This condition occurs at the intersection of the first and second extensor compartments (fig 1). Many, however, contend that the condition is a tenosynovitis of the extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB) tendons. The condition has long been believed to be caused by friction from the overlying extensor pollicis brevis (EPB) and abductor pollicis longus (APL) tendons [8]. Shearing and tensile stresses in the tendons and peritendinous tissues can lead to thickening, adhesions, and cellular proliferation. Subsequently, swelling and proliferation of tenosynovium can cause pain, when these tissues are compressed within the unyielding second extensor compartment.
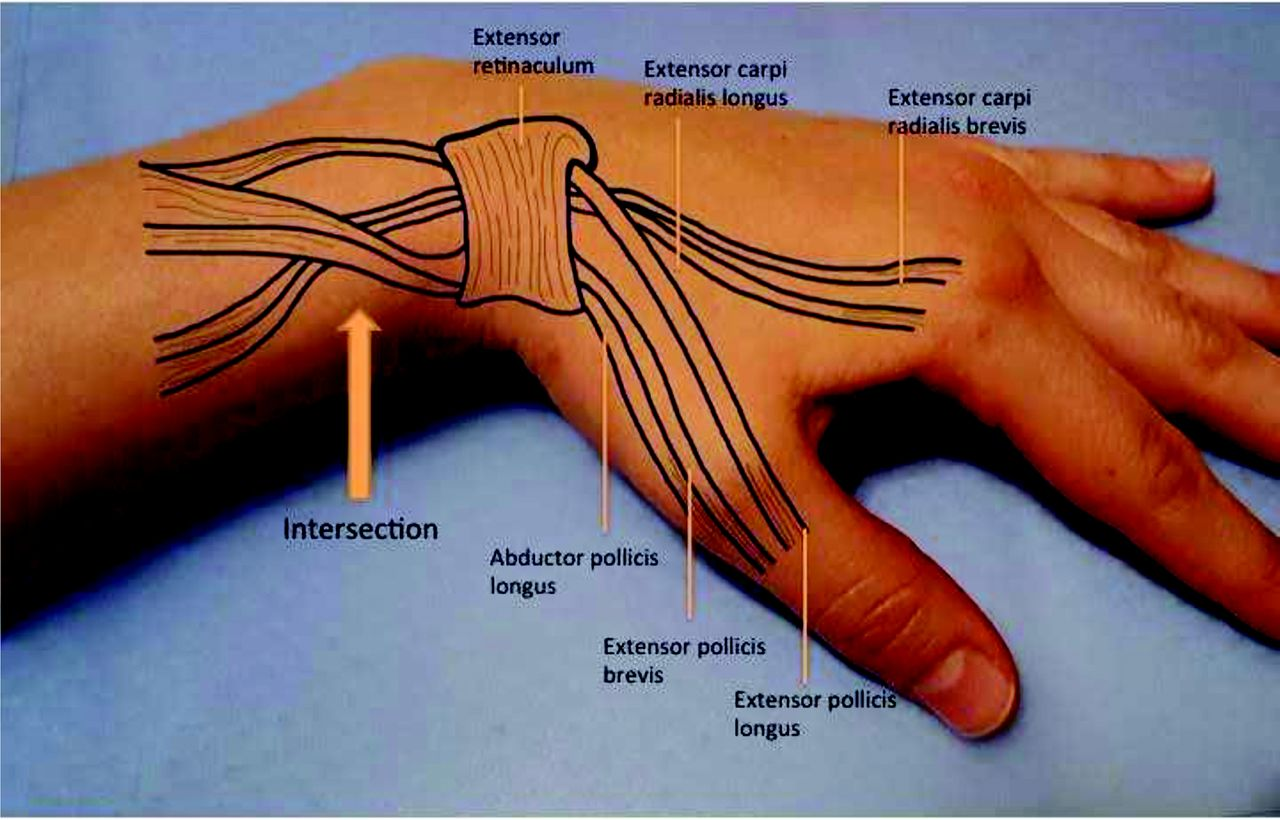
Fig 1.
Clinical Presentation
Patients with intersection syndrome complain of forearm or radial wrist pain. Symptoms are usually exacerbated by repetitive flexion and extension of the wrist.
Examination often shows a discrete swelling at the area of intersection of the tendons. Active or passive wrist motion produces a characteristic crepitus. Other causes of radial forearm pain, such as the following must be excluded:
Thumb CMC arthritis
de Quervain tenosynovitis
Radial sensory nerve irritation (Wartenberg syndrome)
Extensor pollicis longus (EPL) tendinitis
Intersection syndrome is a clinical diagnosis. An ultrasound can easily confirm it. The initial steps for diagnosis include a physical exam of the elbow, wrist, and hand [1,2,9].
The movements of joints above and below the site should be tested. There is a need to look for swelling over the distal forearm since there are some cases that present with a palpable swelling 4 cm - 6 cm proximal to Lister's tubercle. Crepitus at the site of irritation is a very common finding. This finding is specific to intersection syndrome. As the two dorsal compartments cross, supination and pronation of the forearm creates friction resulting in crepitus. Pronation is usually more uncomfortable than supination.[1,2,9].
Intersection syndrome must be differentiated from De Quarvein Syndrome.
De Quarvein Syndrome is a condition that also involves the first dorsal compartment. It is seen below the radial styloid and can be classically tested via the Finkelstein maneuver [1,2].
Plain radiographs and CT are not helpful in the diagnosis of Intersection syndrome. MRI gives an excellent soft tissue picture and helps to confirm the diagnosis. MRI would not be a cost- or time-effective choice [3,6].
Ultrasound can be as specific as MRI in the hands of the skilled user. When observing Intersection syndrome under ultrasound, the ideal image is in the transverse plane. There would be a hypoechoic area in between the two dorsal compartments as they are on top of each other. This would represent swelling/edema that is caused by friction. There may be thickening of the tendon sheaths [3,9].
Differential Diagnosis
The differential diagnosis can include the following:
Dupuytren contracture
Extensor digitorum tenosynovitis
Jammed finger
Jersey's finger
Boutonniere defect
Drummer’s wrist
Mallet finger
Metacarpophalangeal ligament rupture
Ring avulsion injury
Scaphoid fracture
Treatment
Treatment is usually conservative with rest and activity modification. If little or no improvement occurs with conservative treatment corticosteroid injection can produce significant improvement [1,2].
Anti-inflammatory medications are useful for pain relief. The commonly used medications are naproxen, ibuprofen, meloxicam, or diclofenac [2]. Acetaminophen can also be used for pain relief. Rest and activity modification is also effective. Ice can also be used for treatment. A temporary splint for comfort and protection at night may also be beneficial.
When conservative measures are not effective corticosteroid injection can be utilized. The typical injection is a one-to-one mixture of a corticosteroid and local anesthetic.
The injection is done where the first dorsal compartment (abductor pollicis longus and extensor pollicis brevis) is crossed over the second dorsal compartment (extensor carpi radialis brevis/extensor carpi radialis longus) [5]. After the injection is completed, the patient is made to pronate and supinate the wrist. Rehab exercises can be used in tandem with the injection after day 3 to 5. Additionally, prolotherapy is another injectable option. Prolotherapy utilizes a local anesthetic usually lidocaine and a mixture of dextrose in sterile water(5-20%). Prolotherapy creates a proinflammatory state which then triggers the release of growth factors and ultimately collagen deposition, leading to the strengthening of tissue.
In rare, recalcitrant cases surgical debridement and release are indicated.
Surgical Therapy
Surgery can be carried out in cases of intersection syndrome that do not respond to conservative measures [10].
To approach the second extensor compartment a dorsal longitudinal incision is made beginning over the area of swelling and continuing distally 3-4 cm. The dorsal forearm fascia is bluntly dissected and divided longitudinally. Major veins and branches of the radial sensory nerve are protected. The extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB) tendons are completely mobilized by longitudinally incising the extensor retinaculum over the second compartment.
If a bursa is present between the overlying APL and EPB tendons, it is excised.
A thorough tenosynovectomy is performed while elevating and protecting the tendons. This may require mobilization of the APL and EPB, which are then retracted proximally and distally to provide complete access to the second compartment. Repair of the extensor retinaculum is not required. The skin is then closed in a routine fashion.
Compressive dressing and a well-padded volar thumb spica splint are applied with the wrist at 20º of extension for 7-10 days.
At the first postoperative visit, a removable splint is applied and early wrist range-of-motion (ROM) exercises are started. For patients with labor-intensive occupations, occupational therapy is initiated early. The aims of the therapy are strengthening, and obtaining full ROM. The rehabilitation period can last 4-6 weeks.
Complications
Subcutaneous cortisone injections can cause depigmentation in patients who are dark-skinned. These injections can also lead to subcutaneous fat atrophy or necrosis, infection, and tendon rupture. These complications are, however, rare.
Theoretically, the release of the extensor retinaculum can lead to bowstringing of the tendons in extreme wrist extension. However, this potential problem has yet to be reported.
Outcome and Prognosis
A program of conservative management is effective in most patients with intersection syndrome. The patients may need to maintain changes in work or vocational activities to prevent recurrence of symptoms. Individuals who undergo surgery rarely experience recurrence of symptoms.
Unfortunately, in the literature there are no large series documenting the treatment outcome. In one study all eight patients responded to immobilization and corticosteroid injection. Grundberg and Reagan found that about 60% of patients in their practice with intersection syndrome responded to conservative management [11]. They found that 100% of their patients who underwent surgery obtained long-term symptomatic relief.
Controversies
The are some major controversies pertaining to the diagnosis and pathophysiology of intersection syndrome. The doctor must be convinced that the patient's wrist or forearm pain is not due to inflammation or compression of other radial-sided structures, thumb CMC joint, or radial sensory nerve. The location of corticosteroid injection or surgical treatment would differ greatly for these other conditions.
There is some disagreement as to the exact location of tenosynovitis. There is controversy about whether it solely involves the second extensor compartment or represents an abnormal interaction between the tendons of the first and second compartments.
Reference
Browne J, Helms CA. Intersection syndrome of the forearm. Arthritis Rheum. 2006 Jun;54(6):2038.
Servi JT. Wrist pain from overuse: detecting and relieving intersection syndrome. Phys Sportsmed. 1997 Dec;25(12):41-4.
Costa CR, Morrison WB, Carrino JA. MRI features of intersection syndrome of the forearm. AJR Am J Roentgenol. 2003 Nov;181(5): 1245-9.
Descatha A, Leproust H, Roure P, Ronan C, Roquelaure Y. Is the intersection syndrome an occupational disease? Joint Bone Spine. 2008 May. 75(3):329-31.
Wood MB, Dobyns JH. Sports-related extraarticular wrist syndromes. Clin Orthop. 1986 Jan. (202):93-102.
McNally E, Wilson D, Seiler S. Rowing injuries. Semin Musculoskelet Radiol. 2005 Dec. 9(4):379-96.
Tagliafico AS, Ameri P, Michaud J, Derchi LE, Sormani MP, Martinoli C. Wrist injuries in nonprofessional tennis players: relationships with different grips. Am J Sports Med. 2009 Apr. 37(4):760-7.
Wood MB, Linscheid RL. Abductor pollicis longus bursitis. Clin Orthop. 1973 Jun. 93:293-6.
Giovagnorio F, Miozzi F. Ultrasound findings in intersection syndrome. J Med Ultrason (2001). 2012 Oct;39(4):217-20.
Brunton LM, Wilgis EF. A survey to determine current practice patterns in the surgical treatment of advanced thumb carpometacarpal osteoarthrosis. Hand (N Y). 2010 Dec. 5(4):415-22.
Grundberg AB, Reagan DS. Pathologic anatomy of the forearm: intersection syndrome. J Hand Surg [Am]. 1985 Mar. 10(2):299-302.
No comments:
Post a Comment