Myositis Ossificans
Dr. KS Dhillon
Introduction
Myositis ossificans (MO) is an inflammatory ossification of muscle. In 1905, Jones and Morgan [1] raised the question of whether a benign ossifying tumor following trauma was a true inflammatory neoplastic entity. In 1913, Coley [2] reported three cases of traumatic MO. He recognized the difficulty of differentiating it from sarcoma. Ackerman [3] in 1953 argued that MO was a poor designation, established for a group of lesions appearing in soft tissue that may or may not be associated with the periosteum. He sometimes found no associated inflammation. He occasionally found no bone or muscle in the pathophysiologic process. Ackerman [3] not only challenged the literal definition of the term MO but recognized the challenges of distinguishing it from more sinister etiologies.
The term MO has been used to describe a broad spectrum of processes that range from benign solitary lesions to progressive congenital syndromes such as MO progressiva. Lewis [4] in 1923 classified MO into three forms:
Traumatic
Neurotic
Nontraumatic
A year later, Noble [5] classified MO into:
Myositis (fibrous) ossificans progressiva
Traumatic MO circumscripta
MO circumscripta without history of trauma.
The latter includes the pseudomalignant as well as idiopathic forms that are associated with polio, burns, paraplegia, or infections.
Recently, Kransdorf et al [6] defined MO as a solitary, benign, self-limiting, ossifying soft-tissue mass typically occurring within the skeletal muscle. The actual pathophysiological process is not dependent on the associated etiology [7]. The variability in clinical presentation, terminology, imaging characteristics, and histopathology continues to make the diagnosis of MO challenging. Accurate diagnosis is, however, paramount for an optimal treatment plan.
Pathophysiology
The pathophysiology of MO is not completely understood [8,9]. It is believed to occur through the differentiation of fibroblasts into osteogenic cells [10]. Kan et al [11] showed that the cellular mechanism of heterotopic bone formation is the result of the dysregulation of local stem cells in response to tissue injury and subsequent inflammation. There are recent studies that have shown that extraskeletal bone formation may be dependent on a process known as endothelial-mesenchymal transition. Skeletal muscle injury induces a local inflammatory cascade, which leads to the release of cytokines. The cytokines act on the vascular endothelial cells of the skeletal muscle and cause them to undergo endothelial-mesenchymal transition. These endothelial-derived mesenchymal stem cells can differentiate into chondrocytes or osteoblasts. The chondrocytes undergo endochondral bone formation in extraskeletal tissue [12].
Clinically, MO progresses through three parallel clinical, radiographic, and histopathologic stages [7,9,10]. The three overlapping stages of evolution are the early, intermediate, and mature stage [7,9] (table 1).
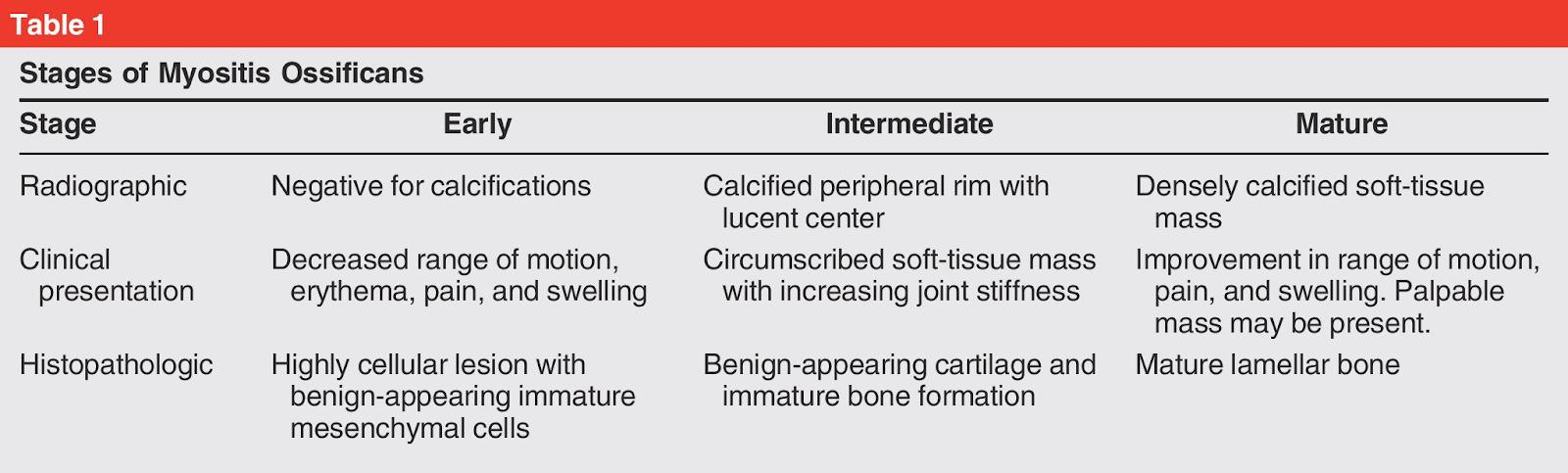
Table 1.
The early stage occurs during the first 4 weeks following injury. It is characterized by an inflammatory cascade that precedes ossification. At this stage, calcifications are not apparent radiographically. Radiographically calcification becomes apparent as the lesion matures through the intermediate stage (4 to 8 weeks) [7,9]. The mature stage that follows is characterized by pronounced peripheral bone formation. Lesion maturation continues during the following months. It culminates in consolidation and, finally, regression [9].
Clinical Presentation
The clinical presentation of MO is quite variable. Most often, the patients can recall a specific injury or repetitive minor trauma. The patients present with pain and joint stiffness following blunt soft-tissue trauma. Young active males are the most commonly affected [7,13]. Repetitive minor trauma can also produce MO. Horseback riders can develop MO in the adductor muscle groups. This condition is commonly known as rider’s bone. Shooters can develop MO in the deltoid. It is commonly referred to as the shooter’s bone [10]. The flexor muscles of the arm and extensor muscles of the thigh are the most commonly affected [7,10].
The patients report muscle pain that persists longer than would be expected for a contusion or simple muscle strain. Pain is due to mechanical irritation of the surrounding tendon, bursa, or joint. When MO compresses the nearby neurovascular structures there can be associated paresthesia, weakness, lymphedema, and venous thromboembolic disease [10]. The symptoms usually abate as the lesion matures [14]. Hence, patients who present late may not have any significant symptoms [9,10,14].
Garland [15] reported that the most common initial sign of MO is a limited range of motion of an adjacent joint. Up to 20% of the patients develop clinically significant functional limitations of movements. Less than 10% of patients develop frank joint ankylosis. In the acute stage edema is usually present. It may be difficult to identify when the muscle injury occurs in large muscle groups [15]. MO of the thigh can produce a decreased range of motion to the knee after injury [16]. Ryan et al [16] reported that there are five risk factors for MO. These include knee motion less than 120 degrees, injury occurring during football, previous quadriceps injury, delay in treatment greater than 3 days, and ipsilateral knee effusion.
Sometimes patients present atypically, especially when the history is not clear. Some of these patients may have suffered unnoticed minor muscle injury. MO has been reported to occur in all ages, including the very young, and in atypical locations such as ribs, hands, feet, head, and neck [17]. Atypical clinical presentation, combined with nonspecific imaging findings, often raises concern about malignancy. Some authors have suggested the use of the more descriptive term pseudomalignant MO [18].
Laboratory Testing
The utility of serum laboratory tests has been examined by several authors [13]. No test is currently diagnostic but several associations have been identified. The serum alkaline phosphatase (SAP) level initially remains normal. With bone formation after 3 weeks the levels become acutely elevated, especially in patients with clinically significant MO [15]. The levels peak (1.3 to 13.4 times normal) at approximately 10 weeks and return to normal by 18 weeks [19]. The SAP level can remain normal even in active lesions, hence the levels cannot be used to determine the maturity or activity of a lesion [19]. In the initial stages of MO acute phase reactants, including the C-reactive protein level, erythrocyte sedimentation rate, and prostagandin-E2 serum level, are elevated [10]. The serum calcium level decreases for a short period and then returns to normal before the rise in SAP [19]. The creatine phosphokinase level is generally elevated if there is involvement of muscle. Unlike SAP it may be predictive for the subsequent development and severity of MO [20].
Imaging
Ultrasonography
An MRI is the preferred modality for the evaluation of soft-tissue masses. Some patients may undergo ultrasonography as an initial diagnostic test. The main value of ultrasonography is in differentiating between cystic and solid lesions. Ultrasonography can also help to detect the zonal pattern of MO, even before calcification is detected on CT [21].
Thomas et al [22] demonstrated the role of ultrasound in the early diagnosis and management of heterotopic bone formation They described three concentric zones. An outer hypoechoic zone that surrounds the lesion, a middle hyperechoic zone that corresponds to the calcifying rim, and a central hypoechoic zone that corresponds to the central fibroblastic stroma. The advantages of ultrasonography include the low cost, lack of radiation exposure, and potential usefulness in the early stages of MO development. Ultrasonography is not recommended as the initial study for suspected MO. If MO is encountered incidentally on ultrasonography, confirmation is recommended with CT.
Radiography
In its mature phase, MO can be diagnosed with radiographs alone. Plain radiographs of MO in the first 2 weeks are typically normal but occasionally demonstrate periosteal reaction [17]. A soft-tissue mass may be seen in the radiographs of acute MO. Soft-tissue calcifications can be seen radiographically at approximately 3 to 4 weeks [9,14]. The calcifications at first appear as amorphous and flocculent. During this phase, the calcifications may simulate osteoid matrix and can have an appearance similar to that of extraskeletal osteosarcoma. MO can also mimic soft-tissue sarcomas associated with calcifications, such as synovial sarcoma. The calcifications usually become more peripherally oriented and coarse in appearance. These calcifications mature during the next several weeks to produce a densely calcified peripheral rim with a lucent center. This typically happens around 6 to 8 weeks. Mature lesions may have a lightly calcified center. This process can take up to 6 months or more. The mature lesions typically run in parallel with the long axis of the muscle. Once the lesion has matured, there is often a radiolucent cleft between the mass and adjacent bone. This can help to differentiate it from parosteal osteosarcoma [22,23]. Mature lesions are sometimes adherent to the adjacent bone. Differentiation from parosteal osteosarcoma may require a CT or an MRI.
Bone Scintigraphy
Bone scintigraphy is of not much use in diagnosing trauma-induced MO, especially when presenting as an isolated soft-tissue mass. However, a bone scan is useful to exclude other inflammatory conditions, such as cellulitis, osteomyelitis, or thrombophlebitis [24]. A bone scan will demonstrate increased uptake in injured muscle because of the presence of calcium salts. It is the most sensitive imaging modality for detecting heterotopic bone formation in the early stages [22,24]. Many authors have found that three-phase bone scintigraphy is more useful in differentiating MO from other inflammatory conditions [22,24].
CT Scan
A CT scan is the best modality for delineating the zonal pattern of calcification. It can be diagnostic even before the characteristic calcification pattern becomes radiographically detectable [25,26]. In the initial stages, the CT scan will show soft-tissue swelling or a low-attenuation soft-tissue mass without associated calcifications. The peripheral rim becomes increasingly calcified as it matures. The central lucent zone is isodense to adjacent muscle [25]. If the peripheral zonal pattern is not evident, it may be difficult to diagnose MO reliably by CT alone.
MRI
MRI is the best modality for imaging soft-tissue masses. An MRI for the evaluation of a soft-tissue mass should be interpreted in conjunction with recent radiographs. This is because calcifications may not be well demonstrated on MRI [27]. In 2007, Papp et al [28] presented the utility of MRI for diagnosing soft-tissue masses. They classified lesions as either determinate or indeterminate based on imaging characteristics and clinical presentation. A determinate lesion can be diagnosed by a good history and physical examination combined with appropriate imaging modalities such as MRI. A lesion in a characteristic location (eg, anterior femoral cortex) supports the diagnosis of MO.
Indeterminate lesions (eg, type of sarcoma) on the other hand require biopsy for an accurate diagnosis. A thorough history and physical examination and a multidisciplinary team approach are useful for optimizing diagnostic accuracy and minimizing risks associated with further evaluation, including biopsy [29].
Although MO can usually be diagnosed definitively by MRI, its appearance can vary depending on the histologic stage [30]. Hence, other diagnostic considerations such as soft tissue sarcoma and abscess must be excluded. In the acute phase, when hematoma is present, MO typically demonstrates a heterogeneous signal intensity on T1-weighted areas of high signal intensity. Fluid-weighted sequences can also be heterogeneous. T2-weighted hyperintensity suggests regions of granulation tissue, edema, and blood products. T2-weighted hypointensity may correspond to calcifications or hemosiderin deposition. When a hematoma is present there is a lack of lesion enhancement. Although intralesional enhancement has been reported in MO, solid or heterogeneous enhancement should raise the suspicion of a sarcoma [31]. A rim of bright T1-weighted signal is often suggestive of peripheral methemoglobin. Surrounding inflammatory edema can also be present. During this stage, gradient-echo sequences can be used to investigate areas of hemosiderin deposition [31].
After the acute phase, the MRI appearance classically demonstrates a lesion that is isointense to slightly hypointense to skeletal muscle on T1-weighted sequences. The fluid-weighted sequences will appear hyperintense to surrounding muscle. At this stage, the surrounding edema may or may not be present. If the zonal pattern of growth, characterized by peripheral low signal intensity is present it would support the diagnosis of MO.
As the lesion progresses, a pattern of mature, lamellar bone becomes better defined. There is low signal intensity on all sequences, and the surrounding edema has resolved. Mature lesions can have areas of internal fat, which correspond to marrow production in the heterotopic bone. If MO is suspected based on MRI, then CT and/or radiographs should be done to confirm the characteristic peripheral mature calcification [31,32].
Differential Diagnosis
The diagnosis of MO is relatively straightforward when it presents with a characteristic history and a clear zonal pattern on imaging. It is, however, not uncommon for the appearance of MO to be suggestive of other lesions which makes the diagnosis challenging (Table 2) [3,7,9,10,18,33].
Nuovo et al [17] reviewed 23 patients who had atypical presentation of MO. Of the 23 patients, 3 patients presented before the age of 10 years. Fifteen lesions were in unusual locations, including the chest wall and the fingers. There was a history of trauma in 8 patients. Two of the 23 patients had constitutional symptoms that led to a presumptive diagnosis of infection. In eight patients the histology suggested a malignant lesion [17]. Hence, a malignancy may be suspected despite advanced cross-sectional imaging and biopsy.
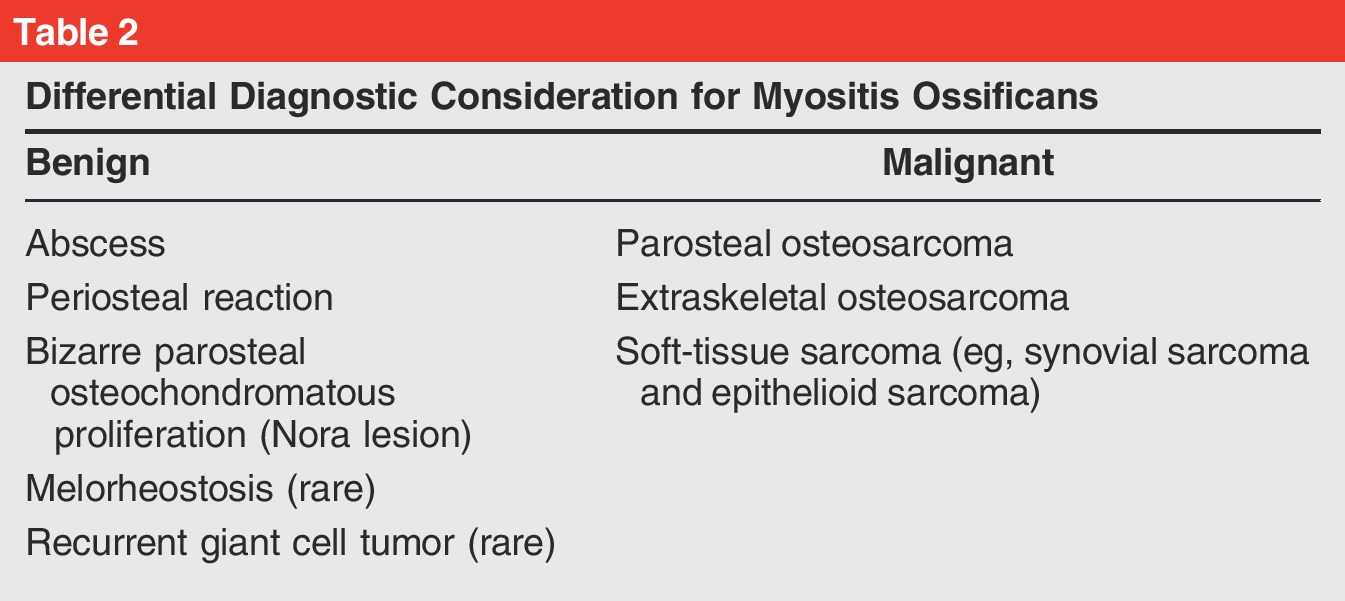
Table 2
In the acute phase of MO, the MRI appearance can mimic a soft-tissue abscess. A soft-tissue abscess will demonstrate a uniform appearance with high signal intensity on T2-weighted sequences, low signal intensity on T1-weighted sequences, and peripheral enhancement on post-contrast images [34]. A CT scan with intravenous contrast demonstrates a bright, rim-enhancing fluid collection, often confirming the suspicion of abscess [34].
It is also important to distinguish MO from a soft-tissue sarcoma. A soft tissue sarcoma can have very similar imaging and pathologic characteristics. A high level of suspicion is often required to make an accurate diagnosis. Atypical presentation such as apparent hematoma lacking ecchymosis, intralesional post-contrast enhancement, and calcifications that lack the characteristic zonal pattern of peripheral ossifications may lead the clinician to favor a sarcoma [31,32]. Up to 58% of patients with synovial sarcoma have calcifications evident on diagnostic imaging and generally lack the peripheral rim of ossification that is seen with MO [35]. A more mature calcification pattern might also be confused with parosteal osteosarcoma on radiographs. It is important to have more advanced cross-sectional imaging [35].
Less commonly encountered conditions that may have soft-tissue calcifications include reactive periostitis and when associated with the surface of the bone, bizarre parosteal osteochondromatous proliferation (Nora lesion). Occasionally, a chronic abscess can develop calcification and thickening of its outer wall, which may appear similar to MO [34].
Melorheostosis is a rare benign sclerotic bone dysplasia that follows a sclerotomal distribution. It is known to have a “myositis-like” variant. The key to differentiating melorheostosis from MO is the identification of the sclerotomal pattern, which is not characteristic of MO. One rare mimicker of MO is a soft-tissue recurrence of a giant cell tumor of bone. Recurrent giant cell tumors of bone in the soft tissues can have peripheral eggshell calcifications, which may appear identical to MO.
Biopsy
When there is a clear history of an inciting event and peripheral calcification on radiographs MO can be classified as a determinate lesion. In early lesions, radiographs are usually nondiagnostic, and MRI findings are usually nonspecific.
Patients who have an indeterminate lesion would require a tissue sample to make a diagnosis before forming a treatment plan. There are several techniques to perform a biopsy. These include fine-needle aspiration, core biopsy, incisional biopsy, and excisional biopsy. Fine-needle aspiration for cytology has been reported to be nondiagnostic. It was unable to rule out sarcoma in some patients with MO. It is generally not recommended when core tissue samples can be obtained for pathologic analysis [29]. CT guidance is best for sampling representative tissue from both the central and peripheral aspects of the lesion.
An incisional biopsy allows direct visualization of the lesion and it offers a large amount of tissue for analysis. It is, however, more invasive compared to close needle biopsies. Incisional biopsies can be used when image guided biopsy is unavailable or when additional tissue is needed. For benign lesions that are small and easily accessible, excisional biopsy can be carried out.
Histopathology
The histopathology of MO progresses from an immature, highly cellular fibroblastic lesion to a mature mass with peripheral lamellar bone [7]. It generally occurs over several weeks and correlates with the development of calcifications on imaging [7,30]. In early lesions, there is mesenchymal metaplasia, intermediate lesions display mixed chondro-osseous differentiation, and mature lesions demonstrate mature bone [9]. In the early stages, microscopically it may be difficult to distinguish MO from sarcoma [7,10]. A mature lesion will present as a thin shell of bone covering a soft red gray central area [7]. It is typically 3 to 6 cm in size. Microscopically, there is a distinct zonal pattern that correlates with the stage of maturity [7,9]. Proliferating fibroblastic tissue and interstitial microhemorrhages can be seen centrally. Some cellular pleomorphism and mitotic activity may also be present [7]. There are areas of immature woven bone mixed with fibroblastic tissue in the intermediate zone. Mature lamellar bone can be seen at the periphery of the lesion. Development of sarcoma in the setting of previous MO has been reported. The ability of MO to transform into sarcoma has been questioned and is not been universally accepted [7].
Treatment
Nonsurgical
The aim of treatment is to minimize symptoms and maximize function. Nonsurgical treatment is usually successful because the disease is self-limiting and the MO often resolves by itself [14,36]. There are no well-designed studies. The observation that MO is more common in patients with bleeding disorders [37] supports the hypothesis that MO is associated with hematoma formation. Therefore, the initial treatment of muscle injury is to control the development of hematoma and maintain function.
For the initial treatment of muscle injury, Järvinen et al [37] recommended a short period of immobilization for 3 to 7 days combined with rest, ice, compression, and elevation. Crutches can be useful to assist with resting the affected area and minimizing hematoma formation [36,37]. Cryotherapy is useful. Ice is applied for 15 to 20 minutes every 30 to 60 minutes. It can reduce the intramuscular blood flow by 50%. Aggressive physical therapy is avoided in the very early stages to prevent exacerbation of symptoms [36,38].
Assisted range of motion exercises, within a pain-free arc of motion, can be started as early as 48 to 72 hours [39]. A gradually progressive exercise program starts with isometric training, followed by isotonic training, and finally dynamic and isokinetic exercises. Fluctuant large and symptomatic hematomas can be aspirated [36]. A study by Lipscomb et al [36] showed that 42 of 42 football players at Vanderbilt University returned to full participation without loss of function after moderate to severe quadriceps contusion. The authors stressed the importance of persistent and early nonsurgical treatment. In the more mature lesions, active range of motion and strengthening exercises are important to maintain and improve joint range of motion and function [10,36,38].
The use of drugs in the prophylaxis of MO after injury is limited. It has been extrapolated from studies examining the development of heterotopic bone formation after hip surgery and pelvic trauma. In a case report of traumatic MO developing in an athlete, two doses of pamidronate were found to improve both the clinical and radiographic findings [40].
Surgical Treatment
Symptomatic lesions that have failed nonsurgical treatment are treated by surgical excision. The aim of surgery is to limit pain and improve function. Surgery is indicated for intractable pain caused by mechanical irritation of nearby tendons, bursa, or joints. Surgery will also be indicated if there is compression of important neurovascular structures, and there is decreased range of motion that compromises activities of daily living [38]. Marginal excision is usually adequate. However, recurrence has been reported [10].
In the past surgical intervention was delayed 6 to 18 months following injury because it was thought that surgery does not alter the maturation process and premature surgery may predispose to recurrence [15]. However, conclusive evidence supporting this is lacking [7,10,13,14,15,38,39]. More recent research has challenged the risk of recurrence with early intervention. A report by Ogilvie-Harris and Fornasier [33] on 26 patients with nontraumatic MO suggested that early excision has minimal risk of recurrence. Garland [15] was of the opinion that the decision when to excise should include the etiology of MO rather than be based solely on chronology. He was of the opinion that surgery should be delayed for 6 months for traumatic MO, 1 year for spinal cord injury patients, and 18 months for head injury patients [15].
The risk of recurrence and severity of MO may be dependent on the initial degree of local soft-tissue trauma. Those who present without disclosing a history of trauma may have suffered a mild injury that went unnoticed. They may do well with early excision if symptomatic. Patients who developed heterotopic bone secondary to severe soft-tissue injury (eg, elbow dislocation), may do better with delayed excision.
Conclusion
Myositis ossificans is a reactive, bone-forming process of soft tissues that occurs after injury. It can mimic malignancy early in its development. The pathophysiology is not completely understood. It likely involves the inappropriate differentiation of mesenchymal stem cells into chondrocytes and osteoblasts in a rich inflammatory environment. Diagnosis is made with a thorough history, physical examination, and imaging modalities. A biopsy may be necessary to confirm the diagnosis in patients with indeterminate lesions. The treatment is usually nonsurgical. It focuses on reducing symptoms and maximizing function. Surgery is needed for lesions that have failed nonsurgical treatment. The optimal timing of surgical excision is once the lesion has reached maturity.
References
Jones R, Morgan D: On osseous formations in muscle due to injury (traumatic myositis ossificans). Archive of the Roentgen 1905; 9(11):245.
Coley WB: Myositis ossificans traumatica: A report of three cases demonstrating the difficulties of diagnosis from sarcoma. Ann Surg 1913;57(3):305–337.
Ackerman LV: Extra-osseous localized non-neoplastic bone and cartilage formation (so-called myositis ossificans): Clinical and pathological confusion with malignant neoplasms. J Bone Joint Surg Am 1958;40(2):279–298.
Lewis D: Myositis ossificans. JAMA 1923;80(18):1281–1287.
Noble TP: Myositis ossificans: A clinical and radiological study. Surg Gynecol Obstet 1924;39:795.
Kransdorf MJ, Meis JM, Jelinek JS: Myositis ossificans: MR appearance with radiologic-pathologic correlation. AJR Am J Roentgenol 1991;157(6):1243–1248.
Folpe AL, Gown AM: Cartilaginous and osseous soft tissue tumors, in Goldblum JR, Folpe AL, Weiss WS, eds: Enzinger & Weiss’s Soft Tissue Tumors, ed 6. Philadelphia, PA, Elsevier, 2014, pp 917–946.
Kan L, Kessler JA: Evaluation of the cellular origins of heterotopic ossification. Orthopedics 2014;37(5):329–340.
Kaplan FS, Glaser DL, Hebela N, Shore EM: Heterotopic ossification. J Am Acad Orthop Surg 2004;12(2):116–125.
Mavrogenis AF, Soucacos PN, Papagelopoulos PJ: Heterotopic ossification revisited. Orthopedics 2011;34(3):177.
Kan L, Liu Y, McGuire TL, et al.: Dysregulation of local stem/progenitor cells as a common cellular mechanism for heterotopic ossification. Stem Cells 2009;27(1):150–156.
Medici D, Olsen BR: The role of endothelial-mesenchymal transition in heterotopic ossification. J Bone Miner Res 2012;27(8):1619–1622.
Beiner JM, Jokl P: Muscle contusion injury and myositis ossificans traumatica. Clin Orthop Relat Res 2002;(suppl 403): S110–S119.
Thorndike A: Myositis ossificans traumatica. J Bone Joint Surg Am 1940;22(2):315–323.
Garland DE: A clinical perspective on common forms of acquired heterotopic ossification. Clin Orthop Relat Res 1991;263:13–29.
Ryan JB, Wheeler JH, Hopkinson WJ, Arciero RA, Kolakowski KR: Quadriceps contusions: West Point update. Am J Sports Med 1991;19(3):299–304.
Nuovo MA, Norman A, Chumas J, Ackerman LV: Myositis ossificans with atypical clinical, radiographic, or pathologic findings: A review of 23 cases. Skeletal Radiol 1992;21(2):87–101.
Jeffreys TE, Stiles PJ: Pseudomalignant osseous tumour of soft tissue. J Bone Joint Surg Br 1966;48(3):488–492.
Orzel JA, Rudd TG: Heterotopic bone formation: Clinical, laboratory, and imaging correlation. J Nucl Med 1985;26(2):125–132.
Singh RS, Craig MC, Katholi CR, Jackson AB, Mountz JM: The predictive value of creatine phosphokinase and alkaline phosphatase in identification of heterotopic ossification in patients after spinal cord injury. Arch Phys Med Rehabil 2003;84(11):1584–1588.
Amendola MA, Glazer GM, Agha FP, Francis IR, Weatherbee L, Martel W: Myositis ossificans circumscripta: Computed tomographic diagnosis. Radiology 1983;149(3):775–779.
Thomas EA, Cassar-Pullicino VN, McCall IW: The role of ultrasound in the early diagnosis and management of heterotopic bone formation. Clin Radiol 1991;43(3):190–196.
Parikh J, Hyare H, Saifuddin A: The imaging features of post-traumatic myositis ossificans, with emphasis on MRI. Clin Radiol 2002;57(12):1058–1066.
Tyler P, Saifuddin A: The imaging of myositis ossificans. Semin Musculoskelet Radiol 2010;14(2):201–216.
Shehab D, Elgazzar AH, Collier BD: Heterotopic ossification. J Nucl Med 2002;43(3):346–353.
Zeanah WR, Hudson TM: Myositis ossificans: Radiologic evaluation of two cases with diagnostic computed tomograms. Clin Orthop Relat Res 1982;168:187–191.
Shirkhoda A, Armin AR, Bis KG, Makris J, Irwin RB, Shetty AN: MR imaging of myositis ossificans: Variable patterns at different stages. J Magn Reson Imaging 1995;5(3):287–292.
Papp DF, Khanna AJ, McCarthy EF, Carrino JA, Farber AJ, Frassica FJ: Magnetic resonance imaging of soft-tissue tumors: Determinate and indeterminate lesions. J Bone Joint Surg Am 2007;89(suppl 3):103–115.
Wakely PE Jr, Almeida M, Frable WJ: Fine-needle aspiration biopsy cytology of myositis ossificans. Mod Pathol 1994;7(1):23–25.
Lacout A, Jarraya M, Marcy PY, Thariat J, Carlier RY: Myositis ossificans imaging: Keys to successful diagnosis. Indian J Radiol Imaging 2012;22(1):35–39.
Kransdorf MJ, Murphey MD: Radiologic evaluation of soft-tissue masses: A current perspective. AJR Am J Roentgenol 2000; 175(3):575–587.
Chen CK, Wu HT, Chiou HJ, et al.: Differentiating benign and malignant soft tissue masses by magnetic resonance imaging: Role of tissue component analysis. J Chin Med Assoc 2009;72(4):194–201.
Ogilvie-Harris DJ, Fornasier VL: Pseudomalignant myositis ossificans: Heterotopic new-bone formation without a history of trauma. J Bone Joint Surg Am 1980;62(8):1274–1283.
Turecki MB, Taljanovic MS, Stubbs AY, et al.: Imaging of musculoskeletal soft tissue infections. Skeletal Radiol 2010;39(10):957–971.
Wilkerson BW, Crim JR, Hung M, Layfield LJ: Characterization of synovial sarcoma calcification. AJR Am J Roentgenol 2012;199(6):W730-4.
Lipscomb AB, Thomas ED, Johnston RK: Treatment of myositis ossificans traumatica in athletes. Am J Sports Med 1976;4(3):111–120.
Järvinen TA, Järvinen TL, Kääriäinen M, Kalimo H, Järvinen M: Muscle injuries: Biology and treatment. Am J Sports Med 2005;33(5):745–764.
Ellerin BE, Helfet D, Parikh S, et al.: Current therapy in the management of heterotopic ossification of the elbow: A review with case studies. Am J Phys Med Rehabil 1999;78(3):259–271.
Pape HC, Marsh S, Morley JR, Krettek C, Giannoudis PV: Current concepts in the development of heterotopic ossification. J Bone Joint Surg Br 2004;86(6):783–787.
Mani-Babu S, Wolman R, Keen R: Quadriceps traumatic myositis ossificans in a football player: Management with intravenous pamidronate. Clin J Sport Med 2014;24(5):e56–e58.
No comments:
Post a Comment