Tibial Shaft Fractures- Management
Dr. KS Dhillon
Introduction
Fractures of the tibia are the most common long bone fractures. The most common fracture of the lower limb occurs at the tibial diaphysis. Knowledge of the methods of treatment of tibial shaft fractures is important, since it is the most common fracture of the long bones, affecting mainly young men. Complications such as reoperation, non-consolidation, and poor consolidation are also relatively common [1].
Open fractures are treated surgically. Close fractures can be treated conservatively or by surgery. All forms of treatment for tibial shaft fractures can be associated with complications [2].
Fracture classification
The most widely used fracture classification is the AO classification. It takes into consideration the region of bone affected, the force involved, and the mechanism of injury. Simple fractures are classified as A, fragmented wedge fractures as B, and multi-fragmented complex fractures as C.
This tibia classification system (type 42) provides good differentiation and understanding of the fracture pattern. It, hence, provides a good relationship between the prognosis and clinical outcome [3]. The type 42 fractures are further subdivided into [4]:
1.42-A simple fracture
42-A1 spiral
42-A2 oblique (≥30˚)
42-A3 transverse (≥30˚)
2.42-B wedge fracture
42-B1 spiral wedge
42-B2 bending wedge
42-B3 fragmented wedge
3.42-C complex fracture
42-C1 spiral
42-C2 segmental
42-C3 irregular
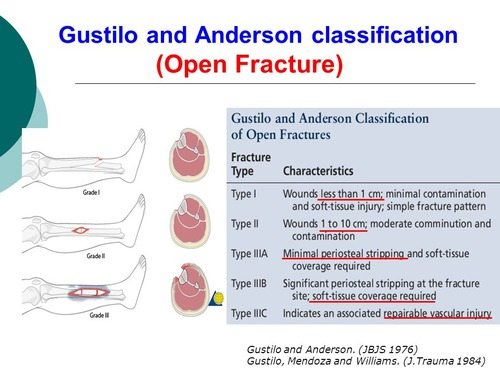
The open fractures are classified according to the Gustilo/Anderson classification [5] as follows:
Diagnosis
Most often patients are able to describe the mechanism of injury. When they have cerebral concussion and loss of consciousness they will not be able to provide history of the mechanism of injury. In such situations, information can be obtained from witnesses who accompany the patient.
Clinical examination will show swelling, inability to move the limb, and deformity in patients with displaced and angulated fractures. AP and lateral view X-rays are usually sufficient. The x-rays should include the knee and the ankle.
Tomography or MRI are not necessary for tibial shaft fractures. The presence of a compartment syndrome should be excluded. The pulses should be felt and duplex sonography carried out if necessary. The consideration of compartment syndrome is a must and it has to be repeatedly evaluated and documented repeatedly.
Treatment
The aims of treatment of tibial shaft fractures are to:
- Reach full weight bearing as fast as possible
- Achieve solid bony union and prevent pseudarthrosis
- Regain full range of the knee and ankle movements
- Prevent infections and further soft tissue damage
Open fractures with precarious blood supply and poor soft tissue cover are vulnerable to complications. Treatment of such fractures remains a challenge for the surgeon treating the patient.
The tibial axis must be realigned, length restored and rotation corrected to obtain a good clinical outcome.
The choice of method of treatment will depend on fracture localization, type of fracture, history of concomitant disorders and the extent of soft tissue damage [6].
Conservative treatment
Tibial shaft fractures that are stable, and are undisplaced can be treated conservatively by cast application. An above knee plaster cast is applied for approximately 4 weeks. The cast is then removed and a functional brace
applied for 8 to 12 weeks [7].
The duration of treatment will depend on the type of fracture. It can be about 8–10 weeks for rotating fractures and at least 12 weeks for transverse fractures [6].
Nicoll [8] analyzed the treatment of 705 tibial fractures. He found that closed treatment achieved overwhelmingly favorable results. He was of the opinion that that surgery was justified only if it could reduce the incidence of deformity, joint stiffness, and delayed union or nonunion.
Suman [9] reported the use of patella bearing cast and early weight-bearing. He claimed rates of union and functional success as high as 100% and praised close treatment for both its simplicity and its limited expense.
Despite the merits of nonoperative management, it has to be noted that not all patients with close tibial shaft fractures are guaranteed a good outcome. Waddell and Reardon [10] in a review of 27 tibia fractures treated by casting found that reduction was lost in 9 patients, 5 required cast wedging, and 3 were treated with late internal fixation. Limb deformity, especially in patients with unstable fractures, is often unavoidable. In a study by Sarmiento et al [11] about 22% of the patients with “acceptable” results after closed treatment, had angulation greater than 5 degrees. The issue is not whether residual deformity occurs with closed methods, but the extent of residual deformity that is considered excessive.
The degree of comminution may directly correlate with eventual limb-length inequality. Digby et al [12] documented severe comminution in 8% of 103 patients treated with cast bracing and they found that shortening of 2 cm or more occurred in 9% of patients.
For conservative treatment of tibia fractures prolonged knee and/or ankle immobilization is usually essential. This often results in joint stiffness. Even with earlier weight-bearing, residual joint stiffness has been reported in about 20% to 30% of patients [10,11]. Digby et al [12] found that, due to residual ankle and subtalar stiffness, 27% of the patients treated with casts could not run long after they had returned to otherwise normal functional status.
The incidence of nonunion after treatment of close tibial fractures can reach 6% [13]. The presence of an intact fibula has been implicated as a major risk factor for tibial delayed union and malunion [14].
Conservative treatment of close tibial-shaft fractures usually produces acceptable results, however, complication rates of up to 66% have been reported [10]. There is a need for comprehensive criteria with which the clinician can select patients who are perhaps better treated operatively. Some of the factors that would suggest that standard conservative treatment methods may be inadequate include:
- Fracture characteristics that retard or inhibit fracture healing
- Fracture instability likely to result in significant deformity
- Associated factors that limit the patient's function or recovery
Prolonged immobilization of the leg in a cast increases the risk of deep vein thrombosis, compartment syndrome, soft tissue injury and regional pain syndrome.
Conservative treatment of tibial fractures by casting is associated with the lowest incidence of infection but on the other hand is associated with a highest incidence of delayed union, malunion and nonunion [2]. The diagnosis of soft tissue injuries and compartment syndrome is also more difficult when the limb is in a cast.
Fracture Healing
The fracture of the tibia can be said to be united in the presence of the following factors:
- The patient's ability to bear weight without pain
- The absence of clinically detectable motion at the fracture site
- The presence of visible bridging callus across the fracture on x rays
Failure of the fracture to unite at 4 to 6 months after injury usually indicates delayed union and failure to unite at 8 to 12 months usually indicates a nonunion [11,15]. When there is compromised fracture healing it should be recognised early and prompt surgical intervention should be considered.
The fracture characteristic most apt to indicate the need for early operative intervention is significant instability, excessive comminution or excessive initial fracture displacement, and severe comminution which is defined as the loss of 50% or more of cortical circumferential continuity. Major displacement, defined as translation of 50% or more of the width of the bone at the fracture site, has been implicated as the cause of up to 50% of delayed unions or nonunions [9].
Axial limb loading provides fracture healing stimulus. When there is significant comminution or displacement of the bone fragments, the time to mobilization or weight-bearing is prolonged thereby depriving the patient of the fracture-healing stimulus of early axial limb loading.
A study by daCosta and Kumar [16] showed that the time to union for the early weight-bearing group was half that for the late weight-bearing group (82 days versus 157 days).
Partial initial stability of the limb in patients with intact fibula may also inhibit fracture healing. Teitz et al [17] in a study of twenty-three patients who were more than 20 years old who were treated for a tibial shaft fracture without a concomitant fibular fracture, six (26 per cent) had delayed union or non-union and six (26 per cent) had varus malunion of the fractured tibia. Sixty-one percent of the patients experienced one or more complications during treatment.
A nonsurgical management course can be initiated and then aborted early if the factors known to be detrimental to healing are recognized and a criterion for more invasive treatment has been established.
Malalignment
The most common complication of nonoperative management of a closed tibial fracture is loss of acceptable alignment. Establishing a threshold for operative intervention is crucial in addressing the issues of limb deformity and its long-term effects on function. However, the extent of limb malalignment that is likely to induce symptoms is controversial [18].
Instability at the fracture site can have an adverse effect on healing limb alignment. Transverse fractures are more stable and are more amenable to closed management and earlier axial loading. Complex fracture patterns demonstrate greater instability and constitute an indication for operative stabilization. The higher-risk fracture patterns include the degree of fracture obliquity, the presence of a spiral pattern, and the extent of fracture comminution. Another indicator of instability is initial fracture displacement of 50% or more of the bone width.
The location of the fracture can also affect the ability to maintain limb alignment with closed methods. Fractures involving the proximal or distal parts of the tibia are especially difficult to immobilize, even when the cast extends to incorporate the adjacent knee and ankle joint. Most tibial fractures occur in the distal third of the bone [19] and angulation can be difficult to control without surgery at this level [20].
Is residual limb deformity actually important in the functional outcome? There are authors who report that a small degree of angular malalignment of the tibia can lead to premature ankle degeneration [21]. The degree of deformity that ultimately becomes functionally significant is not known [22].
Despite the presence of laboratory evidence to the contrary, there are other authors who suggest that a correlation between deformity and poor functional outcome does not exist. Merchant and Dietz [23] in a retrospective review of 20 closed tibial fractures 20 years after injury, found no posttraumatic arthritis in the adjacent knee or ankle, regardless of the residual deformity of the tibia.
Limb shortening, a frequent sequela of closed treatment, is as controversial as angulation with regard to the limits that are deemed acceptable [24].
Operative treatment
Immediate surgical treatment is required for open fractures, compartment syndrome, nerve injury, vessel injury and for patients with multiple injuries.
Several different implants are available for stabilization of the tibia fracture.
All stabilization techniques have both inherent risks and intrinsic benefits. Their appropriateness will ultimately depend on how they compare with closed treatment over time.
Plate fixation of the tibia offers the ability to achieve and maintain anatomic alignment. It has a certain appeal [13,25,26]. Dynamic compression plating and lag-screw fixation have improved the union rates. However, plates are associated with increased soft-tissue morbidity, and early weight-bearing is not always feasible [27]. Plates, like other internal-fixation devices, may sometimes require a separate procedure for hardware removal. The rate of refracture after plate removal has been reported to be as high as 11% [13] which far exceeds the rates obtained with other implants.
External fixation is a less invasive mode of fracture stabilization. It provides better fracture stabilization than a cast and it permits earlier ankle and knee motion. It causes minimal soft tissue injury. Weight-bearing, although permissible, is not always guaranteed, and certain complications such as pin-tract infections may be unavoidable [10]. A period of cast or brace immobilization is often required after removal of the external fixator.
Biomechanical stability and minimally invasive approach at a distance from the fracture are the major advantages of intramedullary nailing. Evidence supports the use of intramedullary nailing for diaphyseal tibial fractures [28,29]. Intramedullary nails can be used for treatment of open fractures if wound closure is performed soon after [29].
Intramedullary nailing is not indicated early in the treatment of patients with severe soft tissue injuries, multiple trauma, thoracic trauma, infection, non-union or children with open growth plate [30].
Intramedullary nailing can be associated with negative effects such as endosteal necrosis and systematic fat embolism [31]. Angular locking screws facilitate the control of rotation, length and axis.
There are some controversies regarding intramedullary nailing. The first is whether intramedullary nails should be inserted with or without reaming. Another is whether intramedullary nails should be locked with locking screws or not.
Intramedullary reaming deposits the debris from reaming at the fracture site. This intramedullary debris acts like an autologous bone graft. The reaming also improves cortical contact with the nail and hence improves stability [32].
Unreamed nailing preserves endosteal blood supply with quicker healing and lower incidence of infection. Blood supply and soft tissue covering are the major problems in tibial shaft fractures. Trauma to endosteal blood supply has been shown to be responsible for the negative effects of intramedullary reaming. For this reason, unreamed intramedullary nailing is widely used in clinical practice in the treatment of open and closed tibial shaft fractures [33].
Court-Brown et al [34] have pointed out that reamed nailing is associated with a significantly lower time to union and a reduced requirement for a reoperation. They recommended not to use unreamed nailing in the treatment of Tscherne C1 tibial fracture with a spiral wedge.
Coles et al [35] also showed superior results with reaming with less delayed union, non-union, mal-union and screw breakage in the treatment of tibia fractures. Their findings were also supported by Forster et al [36]. Lam et al [37] also described beneficial effects of reaming in closed tibial shaft fractures and this was not reflected in open tibial shaft fractures. They concluded that reaming on the one hand disrupts the blood flow to the cortex but on the other hand induces a six fold increase in periosteal blood flow. This reaction does not occur in open fractures and this possibly contributes to the lack of benefit in open fractures.
A Cochrane review by Duan X et al [38] found that there is no clear difference in the rate of major re-operations and complications between reamed or unreamed nailing. There was low quality evidence that reamed nailing reduces the incidence of major reoperations related to non-union in closed fractures and not in open fractures.
Fuchs et al [39] in 2011 published their first short term results using a gentamicin coated intramedullary nail (UTN PROtect®).They showed that these nails can be used both in open and closed fractures and the use of gentamicin coated intramedullary nail was associated with the absence of deep wound infections, good-fracture healing and an increasing weight bearing capacity after six months. Further studies monitoring longer term use of these nails in a larger cohort of patients is, however, required.
To date there is no clear answer as to which form of treatment is the best for closed fractures of the tibial shaft [2]. Without doubt patients with open fractures would require surgery.
Treatment complications
Potential complications following treatment of open and close tibial shaft fractures include post-surgical infection, delayed union, malunion, nonunion, malrotation, compartment syndrome and nerve injury [40-42].
Lau et al [43] reported infective complications in 37 patients (21.4%) out of 173 patients who were treated for open tibia fractures. Thirty-one of their patients (17.9%) sustained post-operative bony complications. They found that patients with Gustilo type III fractures were more than three times as likely to sustain postoperative infective or bony complications, compared to Gustilo type I or II fractures.
Infection following open fractures requires radical surgical intervention to avoid chronic osteitis. Once the medullary cavity is infected intramedullary nails have to be removed and replaced by external fixation. In cases of chronic medullary cavity infection, reaming is the method of choice to open the sequestered parts. Antibiotic treatment is of major importance but it should be accompanied by surgical intervention and radical debridement. Sequestrae have to be removed and can be replaced by autologous bone graft or segmental transportation [44].
Complications are less common with close fractures. Seromas, necrosis and infection with the late onset of osteomyelitis are the most common complications in patients with close fractures [2].
The incidence of compartment syndrome after tibia fractures can range from 1.4% to 48% in various studies [45,46]. Compartment syndrome is more common in young patients [45]. Once compartment syndrome is diagnosed urgent fasciotomy is required with a secondary complete wound closure at a later date.
The combined incidence of delayed and nonunion is lower with operative treatment as compared to close treatment. The combined incidence is 2.6% with plate fixation, 8.0% with reamed nailing, 16.7% with unreamed nailing and 17.2% with closed treatment. The incidence of malunion is also lower with operative treatment as compared with close treatment. It is about 0% with plate fixation, 3.2% with reamed nailing, 11.8% with unreamed nailing and 31.7% with close treatment. Superficial infection is most common with plate fixation (9.0%) compared with 2.9% for reamed nailing, 0.5% for unreamed nailing and 0% for closed treatment. The rates of reoperation ranges from 4.7% to 23.1% [2].
Prognosis
Prognosis following tibial shaft fractures correlates with injury severity, extent of soft tissue damage and associated injuries. The surgical treatment also depends on these factors. Unreamed intramedullary nailing allows the patient to weight bear early. Infection rates can vary from 0.5% for reamed nails, 9% with plate fixation and 21.7% in patients with open fracture. Tibia fractures remain vulnerable to complications and often require secondary surgery. According to Bhandari et al. there are three main indicators of revision surgery i.e open fractures, transverse fracture pattern and postoperative fracture gap [47]. In the presence of all three risk factors reoperation rate can be as high as 90%.
Conclusion
Tibial shaft fractures can be treated with cast immobilization or a one or two-stage surgical treatment. Intramedullary nailing is probably the most widely used technique for the treatment of shaft fracture. In haemodynamically unstable patients early osteosynthesis is important. External fixation is indicated in patients with multiple trauma, open fractures, and in those with severe soft tissue injuries. Intramedullary nailing reduces the need for revision surgeries and reduces the incidence of non-unions and infections as compared to external fixation. There is also a reduced risk of revision surgeries with reamed nails as compared to unreamed nails.
References
- Freedman EL, Johnson EE. Radiographic analysis of tibial fracture malalignment following intramedullary nailing. Clin Orthop Relat Res. 1995;(315):25-33.
- Coles CP, Gross M. Closed tibial shaft fractures: management and treatment complications. A review of the prospective literature. Can J Surg. 2000 Aug;43(4):256-62.
- Swiontkowski MF, Agel J, McAndrew MP, Burgess AR, MacKenzie EJ. Outcome validation of the AO/OTA fracture classification system. J Orthop Trauma. 2000;14(8):534-41.
- MÜLLER et al. The comprehensive classification of fractures of long bones. Springer, 1990.
- GUSTILO et al. Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. J. Trauma, 24: 742–746, 1984.
- MAYR, E.: (Tibial fractures). Chirurg, 73: 642–661; quiz 662–663, 2002.
- SARMIENTO, A., et al.:Tibial shaft fractures treated with functional braces. Experience with 780 fractures. J. Bone Jt Surg. 71-B: 602–609, 1989.
- Nicoll EA: Fractures of the tibial shaft: A survey of 705 cases. J Bone Joint Surg Br 1964;46:373-387.
- Suman RK: The management of tibial shaft fractures by early weight bearing in a patella tendon bearing cast: A comparative study. J Trauma 1977;17:97-107.
- Waddell JP, Reardon GP: Complications of tibial shaft fractures. Clin Orthop 1983;178:173-178.
- Sarmiento A, Sobol PA, Sew Hoy AL, et al: Prefabricated functional braces for the treatment of fractures of the tibial diaphysis. J Bone Joint Surg Am 1984; 66:1328-1339.
- Digby JM, Holloway GMN, Webb JK: A study of function after tibial cast bracing. Injury 1983;14:432-439.
- Jensen JS, Hansen FW, Johansen J. Tibial shaft fractures. A comparison of conservative treatment and internal fixation with conventional plates or AO compression plates. Acta Orthop Scand. 1977;48(2):204-12. doi: 10.3109/17453677708985136. PMID: 868506.
- Teitz CC, Carter DR, Frankel VH: Problems associated with tibial fractures with intact fibulae. J Bone Joint Surg Am 1980;62:770-776.
- Johner R, Wruhs O: Classification of tibial shaft fractures and correlation with results after rigid internal fixation. Clin Orthop 1983;178:7-25.
- daCosta GIB, Kumar N: Early weightbearing in treatment of fractures of the tibia. Injury 1979;11:123-131.
- Teitz CC, Carter DR, Frankel VH: Problems associated with tibial fractures with intact fibulae. J Bone Joint Surg Am 1980;62:770-776.
- Bridgman SA, Baird K: Audit of closed tibial fractures: What is a satisfactory outcome? Injury 1993;24:85-89.
- Bridgman SA, Baird K. Audit of closed tibial fractures: what is a satisfactory outcome? Injury. 1993 Feb;24(2):85-9. doi: 10.1016/0020-1383(93)90194-b. PMID: 8505133.
- Bone LB, Johnson KD: Treatment of tibial fractures by reaming and intramedullary nailing. J Bone Joint Surg Am 1986;68:877-887.
- McKellop HA, Llinás A, Sarmiento A. Effects of tibial malalignment on the knee and ankle. Orthop Clin North Am. 1994 Jul;25(3):415-23. PMID: 8028885.
- Kristensen KD, Kiaer T, Blicner J: No arthrosis of the ankle 20 years after malaligned tibial-shaft fracture. Acta Orthop Scand 1989;60:208-209.
- Merchant TC, Dietz FR. Long-term follow-up after fractures of the tibial and fibular shafts. J Bone Joint Surg Am. 1989 Apr;71(4):599-606. PMID: 2703519.
- Hooper GJ, Keddell RG, Penny ID: Conservative management or closed nailing for tibial shaft fractures: A randomised prospective trial. J Bone Joint Surg Br 1991;73:83-85.
- Zagorski JB, Latta LL, Finnieston AR, et al: Tibial fracture stability: Analysis of external fracture immobilization in anatomic specimens in casts and braces. Clin Orthop 1993;291:196-207.
- Schmidt A, Rorabeck CH: Fractures of the tibia treated by flexible external fixation. Clin Orthop 1983;178:162-172.
- Trafton PG: Closed unstable fractures of the tibia. Clin Orthop 1988;230:58-67.
- BHANDARI, M., et al., Reamed versus nonreamed intramedullary nailing of lower extremity long bone fractures: a systematic overview and meta-analysis. J. Orthop. Trauma, 14: 2–9, 2000.
- BHANDARI, M., et al. Treatment of open fractures of the shaft of the tibia. J. Bone Jt Surg., 83-B: 62–68, 2001.
- RÜEDI, T.P., BUCKLEY, R.E., MORAN, C.G.: AO principles of fracture management. Vol. 1, 2007.
- HOGEL, F., et al.: Fracture healing after reamed and unreamed intramedullary nailing in sheep tibia. Injury, 42: 667–674, 2011.
- REYNDERS, P.A., BROOS, P.L.: Healing of closed femoral shaft fractures treated with the AO unreamed femoral nail. A comparative study with the AO reamed femoral nail. Injury, 31: 367–371, 2000.
- MÜLLER, C.A., MORAKIS, P.H., STROHM, P.C., PFISTER, U.: Intramedullary nailing of the tibia: current status of primary unreamed intramedullary nailing. Part 2: results in open fractures. Injury, 3(Suppl.3): 44–54, 1999.
- COURT-BROWN, C.M., et al.: Reamed or unreamed nailing for closed tibial fractures. A prospective study in Tscherne C1 fractures. J. Bone Jt Surg., 78-B: 580–583, 1996.
- COLES, C.P., GROSS, M.: Closed tibial shaft fractures: management and treatment complications. A review of the prospective literature. Can. J. Surg., 43: 256–262, 2000.
- FORSTER, M.C., BRUCE, A.S., ASTER, A.S.: Should the tibia be reamed when nailing? Injury, 36: 439–444, 2005.
- LAM, S.W., et al.: Systematic review shows lowered risk of nonunion after reamed nailing in patients with closed tibial shaft fractures. Injury, 41: 671–675, 2010.
- Duan X, Al-Qwbani M, Zeng Y, Zhang W, Xiang Z. Intramedullary nailing for tibial shaft fractures in adults. Cochrane Database Syst Rev. 2012 Jan 18;1:CD008241. doi: 10.1002/14651858.CD008241.pub2. PMID: 22258982.
- FUCHS, T., et al.: The use of gentamicin-coated nails in the tibia: preliminary results of a prospective study. Arch. Orthop. Trauma Surg., 131: 1419–1425, 2011.
- Metsemakers WJ, Handojo K, Reynders P, Sermon A, Vanderschot P, Nijs S. Individual risk factors for deep infection and compromised fracture healing after intramedullary nailing of tibial shaft fractures: a single centre experience of 480 patients. Injury 46(4), 740–745 (2015).
- Auston DA, Meiss J, Serrano R et al. Percutaneous or open reduction of closed tibial shaft fractures during intramedullary nailing does not increase wound complications, infection or nonunion rates. J. Orthop. Trauma 31(4), 215–219 (2017).
- Johal H, Bhandari M, Tornetta P 3rd. Cochrane in CORR (R ): Intramedullary nailing for tibial shaft fractures in adults (Review). Clin. Orthop. Relat. Res. 475(3), 585–591 (2017).
- Lua et al. Complications of Open Tibial Fracture Management: Risk Factors and Treatment. Malaysian Orthopaedic Journal. 2017 Vol 11 No 1.
- SONG, H.R., et al.: Comparison of internal bone transport and vascularized fibular grafting for femoral bone defects. J. Orthop. Trauma, 17: 203–211, 2003.
- PARK, S., et al.: Compartment syndrome in tibial fractures. J. Orthop. Trauma, 23: 514–518, 2009.
- WOLL, T.S., DUWELIUS, P.J.: The segmental tibial fracture. Clin. Orthop. Relat. Res., 281: 204–207, 1992.
- BHANDARI, M., et al.: Predictors of reoperation following operative management of fractures of the tibial shaft. J. Orthop. Trauma, 17: 353–361, 2003.