Tarsal Tunnel Syndrome
DR KS Dhillon
Introduction
The tarsal tunnel syndrome was first described by Keck and Lam in 1962. It is a condition that is caused by compression of the tibial nerve or its associated branches as the nerve passes beneath the flexor retinaculum at the level of the ankle or distally [1,2,3,4,5,6,7,8]. It is similar to the carpal tunnel syndrome of the wrist.
It is a compression neuropathy that manifests with pain and paresthesias that radiate from the medial side of the ankle distally and, occasionally, proximally. The signs and symptoms of tarsal tunnel syndrome can be due to a variety of causes, that can be categorized as intrinsic, extrinsic, or tensioning factors.
Extrinsic causes include external trauma due to stretch injury, crush injury, fractures, dislocations of the ankle and hindfoot, and severe ankle sprains.
Intrinsic causes of the neuropathy include space-occupying masses, bony prominences, localized tumors, and a venous plexus within the tarsal canal.
Nerve tension caused by a valgus foot can produce symptoms that are similar to those of nerve compression.
The symptoms will vary from individual to individual. Sensory disturbance varies from sharp pain to loss of sensation. There can be atrophy of the intrinsic muscles of the foot. There can be a gait abnormality with overpronation and a limp due to pain on weightbearing.
A hindfoot valgus deformity can aggravate the symptoms of tarsal tunnel syndrome because the deformity can increase tension due to an increase in foot eversion and dorsiflexion.
Anatomy
The tarsal tunnel is a fibro-osseous space that is located on the posteromedial aspect of the ankle (fig1). It provides a passageway for tendons, nerves, and vessels to travel between the posterior leg and the foot. Its floor is a concave surface formed by the medial aspect of the tibia, talus, and the calcaneus. It is converted into a tunnel by the flexor retinaculum. The flexor retinaculum spans obliquely between the medial malleolus and the medial tubercle of the calcaneus to form the roof. It is continuous with the deep fascia of the leg and foot.
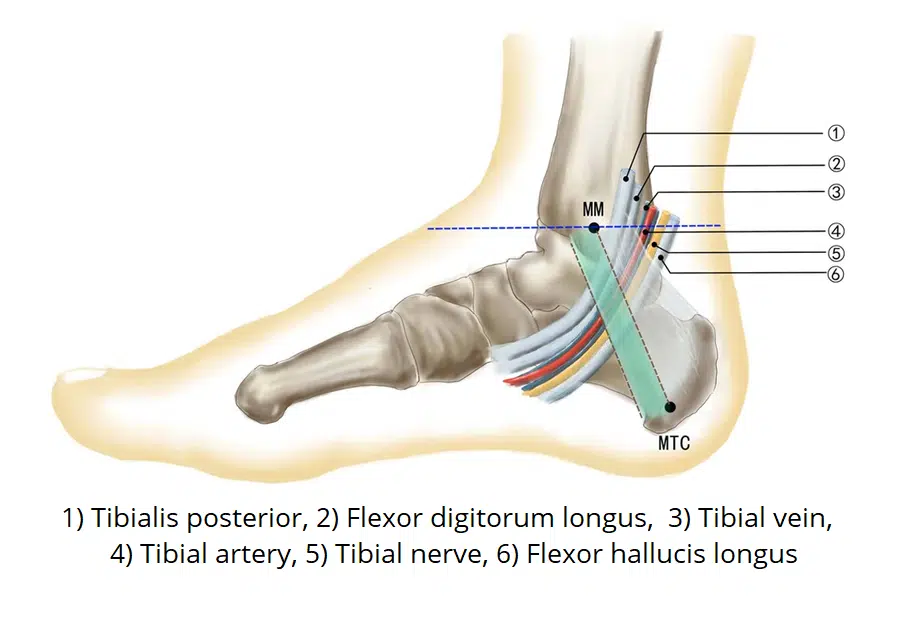
Fig 1.
The tarsal tunnel acts as a passageway for nerves, tendons, and vessels to travel between the posterior leg and the foot. Its contents (anterior to posterior) are:
Tibialis posterior tendon
Flexor digitorum longus tendon
Posterior tibial artery and vein
Tibial nerve
Flexor hallucis longus tendon
The tunnel is divided into four fibrous compartments, one containing the neurovascular structures and the other three containing the muscle tendons.
Pathophysiology
Tarsal tunnel syndrome is a compression neuropathy of the tibial nerve that is situated in the canal. The symptoms of tension and compression neuropathies are similar. Hence differences in these conditions cannot be simply identified by the symptoms alone. In some patients compression and tension neuropathies may coexist.
In 1973 Upton and McComas described the double-crush phenomenon. According to them local damage to a nerve at one site along its course may sufficiently impair the overall functioning of the nerve cells, such that the nerve cells become more susceptible to compression trauma at distal sites.
The nerves are responsible for transmitting afferent and efferent signals along their length. They are also responsible for moving their nutrients, which are essential for optimal functioning. The movement of these intracellular nutrients is accomplished through a type of cytoplasm within the nerve cell called axoplasm. The axoplasm moves along the entire length of the nerve. If the flow of the axoplasm is blocked, the nerve tissue that is distal to the site of compression is nutritionally deprived and more susceptible to damage [9].
Upton and McComas were of the opinion that a high proportion (75%) of patients with one peripheral nerve lesion did have a second lesion elsewhere. Both lesions contributed to the patient's symptoms. These lesions were originally studied in patients with brachial plexus injury. Patients with brachial plexus injuries had a higher incidence of carpal tunnel neuropathy. The double-crush phenomenon can also be seen in the feet. In patients with compression of the S1 nerve root, there is an increased likelihood of compression neuropathy in the tarsal canal.
Etiology
There are several causes of tarsal tunnel neuropathy. Soft-tissue masses can cause compression neuropathy of the posterior tibial nerve. These masses include the following:
Neoplasms within the tarsal canal
Nerve sheath and nerve tumors
Lipomas
Tendon sheath ganglia
Varicose veins
Parkhurst et al [10] reported three cases of tarsal tunnel syndrome. The tarsal tunnel syndrome in these patients was caused by an accessory flexor digitorum longus.
Tibial nerve entrapment is common in patients with diabetes. Bony prominences and exostoses can also cause this disorder. A study by Daniels et al [11] showed that a valgus deformity of the rearfoot may contribute to the neuropathy by increasing the tensile load on the tibial nerve.
Prognosis
Properly performed decompression of the tarsal tunnel can produce satisfactory results. After the decompression, an initial marked decrease in pain and paresthesias can occur. This is followed by a further reduction of symptoms. Sometimes complete resolution of symptoms may not be possible because the disorder has numerous etiologies and because there is irreversible nerve damage. An increase in pain after decompression, however, is very rare.
Studies by Mann [12] show that approximately 75% of patients who undergo surgical decompression have appreciable pain relief, and 25% of the patients obtain little or no relief. He also stated that a repeat surgical exploration of a previous tarsal canal release rarely produces appreciable benefit to the patient.
Gondring et al [13] carried out a prospective evaluation of 46 consecutive patients (56 feet) who underwent nonoperative and surgical treatment for tarsal tunnel syndrome. They documented pain intensity before and after treatment with the Wong-Baker FACES Pain Rating Scale.
They found that patients who had successful nonoperative treatment experienced a significant reduction in overall pain intensity in the medial calcaneal, medial plantar, and lateral plantar nerve regions. Pts who had surgical treatment had significantly reduced pain in the medial calcaneal and medial plantar nerve regions but not in the lateral plantar nerve area. The pretreatment motor nerve conduction latency was significantly greater in surgically treated patients as compared to those who had nonoperative treatment.
Antoniadas et al [14] performed a literature review of posterior tarsal tunnel syndrome. They found that accurate diagnosis required proper clinical, neurologic, and neurophysiologic examinations. The success rates of operative treatment were between 44% to 91%. The results were better in idiopathic cases than in posttraumatic cases. If surgery failed, reoperation was indicated only in patients with inadequate release.
McSweeney et al [15] conducted a rigorous review of tarsal tunnel syndrome that included the Cochrane Neuromuscular Group's Specialized Register, as well as AMED, MEDLINE, EMBASE, CINAHL, Physiotherapy Evidence Database (PEDro), Biomed Central, Science Direct, and Trip Database (1972-2015). Their study found that there was limited high-level robust evidence to guide and refine the clinical management of tarsal tunnel syndrome.
Yu et al [16] studied 107 patients with tarsal tunnel syndrome and found that the efficacy of surgical treatment of tarsal tunnel syndrome was correlated with the cause of the syndrome, the nerve bundles involved, the operative method employed, and whether neurolysis of the epineurium was performed.
A study by Lalevée et al [17] of 45 patients with a mean follow-up of 3.6 ± 1.8 yrs evaluated surgical results in relation to the etiology of tarsal tunnel syndrome. They divided subjects into the following three groups [17] :
Group 1 - Permanent intra- or extra tunnel space-occupying compressive structure
Group 2 - Intermittent intratunnel venous dilatations
Group 3 - Idiopathic tarsal tunnel syndrome
The main endpoint was a subjective postoperative improvement on the Likert scale. Patients in group 1 reported greater improvement than patients in groups 2 and 3. This suggests that surgical treatment of this syndrome yields better results when the etiology involves structural compression.
Clinical presentation
History
While taking a history of the patient with suspected peripheral neuropathy a careful review of the past medical history, with attention to systemic diseases that can be associated with peripheral neuropathy, such as hypothyroidism and diabetes, is necessary.
There are several medications that can cause peripheral neuropathy. These include colchicine, metronidazole, lithium, nitrous oxide, phenytoin, cimetidine, disulfiram, chloroquine, amitriptyline, thalidomide, cisplatin, pyridoxine, and paclitaxel. These drugs can produce distal symmetric sensorimotor neuropathy.
Patients should be questioned about their exposure to the human immunodeficiency virus (HIV), vitamin use, Lyme disease, and exposure to leprosy. A family history of the presence of hammer toes, muscle weakness, gait abnormalities, and cavus foot, may indicate a long-standing or familial neuropathy.
Physical Examination
Patients usually present with vague symptoms of foot pain. This pain can sometimes be confused with plantar fasciitis. Examination usually shows tenderness over the nerve. There can be paresthesias and numbness of the foot in the distribution of the tibial nerve. In some cases, atrophy of the intrinsic foot muscles may be present. Dorsiflexion and eversion of the foot may cause symptoms to increase.
The Tinel and Phalen sign may often be present posterior to the medial malleolus. Symptoms usually subside with rest, though they typically do not disappear altogether. Physical examination may show reduced sensitivity to pinprick, light touch, and temperature.
X-rays of the limb may show osteopenia, thinning of the phalanges, or evidence of neuroarthropathy (eg, Charcot disease). Additionally, trophic changes may include loss of hair, pes cavus, and ulceration. These findings are most prominent in patients with leprosy, diabetes, amyloid neuropathy, or hereditary motor sensory neuropathy with prominent sensory involvement. Perineural thickening may be seen in patients with leprosy and amyloid neuropathy.
Differential Diagnoses
The differential diagnosis for tarsal tunnel syndrome includes the following:
Stress fractures of the hindfoot, particularly the calcaneus
Herniated spinal disk
Plantar fasciitis
Peripheral neuropathies, such as those caused by alcoholism or diabetes
Inflammatory arthritides, such as rheumatoid arthritis or Reiter syndrome
Laboratory Studies
Patients with diabetes mellitus develop a distal, symmetric motor, and sensory polyneuropathy. This axonal neuropathy is due to the degeneration of the distal axons. Diabetes also produces a neuropathy due to microangiopathy. This results in a proximal, asymmetric mononeuropathy primarily affecting motor nerves. The initial investigation includes urinalysis and tests of the fasting serum glucose level, hemoglobin A1c, blood urea nitrogen, creatinine, complete blood count, erythrocyte sedimentation rate, and vitamin B12 levels.
In patients with Reiter syndrome the arthritis typically affects the knees, ankles, and feet, causing pain and swelling. The wrists, fingers, and other joints are less often affected. The patients commonly develop inflammation where the tendon attaches to the bone, a condition called enthesopathy. Enthesopathy can produce heel pain and shortening and thickening of fingers and toes. Some of these patients also develop heel spurs that are associated with chronic or long-lasting foot pain.
Reiter syndrome usually affects men between the ages of 20 and 40 years. It is the most common type of arthritis that affects young men. Among men younger than 50 years, about 3.5 per 100,000 develop Reiter syndrome each year. About 3% of all men with a sexually transmitted disease develop Reiter syndrome. Women can also develop this disorder, though less often than men. The features in women are often milder and more subtle.
About 80% of the affected patients are positive for human leukocyte antigen (HLA)-B27. Only 6% of the individuals who do not have Reiter syndrome have the HLA-B27 gene.
To rule out underlying systemic arthritic conditions, ESR, rheumatoid factor (RF), and antinuclear antibody (ANA) serology should be performed. Patients with rheumatic diseases, including Reiter syndrome, will have an elevated ESR. However, in Reiter syndrome, the results of RF and ANA testing are negative. HLA-B27 typing may be useful in differentiating this seronegative arthropathy from other arthritides.
Pressure atrophy of nerve fibers can cause peripheral neuropathy in patients with generalized amyloidosis. The central nervous system is not affected except in areas that lack a blood-brain barrier, such as the pineal gland and choroid plexus. Nerve biopsy is helpful in some cases to diagnose sarcoidosis, leprosy, amyloid neuropathy, and leukodystrophies.
Imaging Studies
Ultrasonography (US) and magnetic resonance imaging (MRI) may be useful modalities in suspected cases of soft-tissue masses and other space-occupying lesions in the tarsal tunnel. MRI is useful in assessing flexor tenosynovitis and unossified subtalar joint coalitions [18]. A small study by Fantino et al [19] found measurement of the axial cross-section area of the tibial nerve between the posteromedial tarsal tunnel and a point 10 cm above the tunnel with US to be a key data point in diagnosing tarsal tunnel syndrome.
X-rays are useful in evaluating the patient's underlying foot structure, bony masses, osteophytes, fractures, and subtalar joint coalition.
Electromyography and Nerve Conduction Velocity Studies
Nerve conduction velocity (NCV) and electromyography (EMG) studies are initial tools in evaluating suspected cases of tarsal tunnel syndrome and in confirming the presence of neuropathy. Additionally, the type of nerve fiber (motor, sensory, or both) and the pathophysiology (axonal vs demyelinating and symmetric vs asymmetric) can be differentiated with the information obtained from NCV or EMG.
EMG studies may show prolonged posterior tibial nerve distal latency to the abductor hallucis or abductor digiti quinti muscles. This may also be accompanied by low motor amplitude or absent responses in either of these muscles. The lateral or medial plantar sensory action potentials may be affected with prolonged latency, slowed velocity, and decreased amplitude. In patients with advanced tarsal tunnel syndrome, the sensory action potentials may be unobtainable.
Needle examination of the abductor hallucis or abductor digiti quinti muscles may show denervation. There should be sparing of the posterior tibial muscles above the tarsal tunnel (posterior tibialis). The lumbosacral paraspinal muscles should also be intact.
The EMG and NCV testing values include the following:
Prolonged distal motor latency - Terminal latencies of the abductor digiti quinti muscle (lateral plantar nerve) longer than 7.0 ms are abnormal
Fibrillations in the abductor hallucis muscle may be present
Terminal latencies of the abductor hallucis muscle (medial plantar nerve) longer than 6.2 ms are abnormal
Repeat EMG studies are performed 6 months after the surgery to assess the physiologic success of the decompression procedure. A decrease may be noted in the distal latencies.
The results of NCV studies may be normal in patients with small-fiber neuropathies. Lower-extremity sensory responses may be absent in normal elderly patients. Hence, electrodiagnostic testing should not be a substitute for a good clinical examination.
Histological Findings
In most cases of neuroma in continuity, the nerve has an intact perineural sheath. There can be nerve swelling due to chronic nerve compression and irritation. The proliferation of fibrous tissue causes nerve compression.
Ganglion cysts that cause compressive peripheral neuropathies are uncommon, but when combined, they are not uncommon. The source and cause of ganglion cysts remains unsettled. One theory was fibrillar degeneration of collagen, with accumulation of intracellular and extracellular mucin. If seen during surgery, these lesions must be removed in toto as part of nerve decompression.
Management
The clinical result after surgical decompression of the tibial nerve is good. The absence of positive electrodiagnostic findings does not rule out the possibility that decompression may be successful in treating the symptoms of tarsal tunnel syndrome.
Surgery is contraindicated in patients who are not medically fit for surgery.
There are several conditions that may mimic or coexist with tarsal tunnel neuropathy. Patients with such conditions do not improve after surgical decompression.
There are some concerns regarding whether decompression of the tibial nerve in patients with marked pes planovalgus deformity may cause a deleterious effect. This is because decompression of the medial retinacular compartment may be associated with an increase in nerve tension. A joint stabilization procedure may be a necessary adjunct in determining long-term postoperative success. There are no studies performed to assess the long-term efficacy of decompression and stabilization, decompression and orthoses management, and decompression alone.
Tibial nerve entrapment is common in diabetic patients, causing neuropathic complaints and sensory disturbances. There have been suggestions that surgical treatment of tarsal tunnel syndrome may help prevent diabetic foot disease and thus reduce the risk of amputation [20].
Medical Therapy
In the initial stages, tarsal tunnel syndrome can be treated with local anesthetic and steroid injections. These injections can help reduce the pain. The syringe needle has to be carefully placed to prevent injury to the nerve. Physical therapy may be of some value in reducing local soft-tissue edema, thereby reducing pressure on the compartment.
If there is a contracture of the triceps surae muscles, stretching exercises should be initiated. A well-designed foot orthosis may reduce tension on the tibial nerve by decreasing the load on the medial column in patients with pes planovalgus foot.
The night splints with the foot in plantarflexion and varus may be used in patients with a valgus foot. Such treatment has not been shown to have long-term efficacy in well-controlled comparison studies, but it is commonly used in clinical practice [21].
Surgical Therapy
When conservative therapy fails surgical intervention may be warranted. Space-occupying masses are removed. The neurilemoma of the tibial nerve may have to be removed.
If the nerve impingement is due to adhesions and scar tissue external neurolysis of the nerve may be necessary. If scarring or entrapment encapsulates the nerve tissue a release of the epineurium will also have to be carried out.
The tarsal tunnel decompression can be carried out by an endoscopic technique [22]. Krishnan reported a case series where he used an endoscopic technique in the tarsal tunnel in 24 patients. Six of the patients were females and 18 were males. The age ranged from 28-82 years. The mean age at surgery was 54.6 years [23]. All the cases were unilateral.
Of the 24 patients, 14 were idiopathic and 10 had posttraumatic tarsal tunnel syndrome [23]. Twenty-one patients had the classic presentation of tarsal tunnel syndrome, two had the algetic form and three had the distal variant. Thirteen patients had diabetes mellitus, two had polyneuropathy, and five had peripheral vascular occlusive disease.
Evaluation of the results in these patients was conducted according to Bishop's five-scale system i.e. excellent/very good/good/moderate/poor. The follow-up ranged from 6 months to 6 years with a mean of 2.5 years. Of the 24 patients, eight had excellent results, 10 very good, four good, and two poor. The two patients with poor results had relapses. Of the 13 patients with concomitant diseases, all but two improved. Only one had excellent results, six had very good results, four good, and two poor. The protective sensation recovered in all patients.
Iborra Marcos et al [24] described an ultra-minimally invasive approach to decompression of the tibial nerve under ultrasonographic guidance. They found it to be effective.
Preparation for surgery
The patient is placed in either the lateral recumbent position or the supine position to facilitate exposure of the medial aspect of the foot to be operated on. A pneumatic tourniquet is applied before the surgery.
Operative details
A curved incision is made approximately 1 cm posterior to the distal tibia and it is extended to the plantar aspect of the foot paralleling the shaft and the medial malleolus and it is gradually curved towards the sustentaculum tali. Mini-open incisions for tarsal tunnel release can also be used with outcomes as good as the standard approach [25].
The retinaculum is identified and carefully released. The posterior tibial nerve is identified, and visualized, along its course until its bifurcation at the porta pedis. Care should be taken to avoid cutting the small calcaneal branches that arise from the posterior tibial nerve. These branches are often surrounded by fatty tissue and may be difficult to visualize.
The medial and lateral plantar branchs of the posterior tibial nerve should be identified. The medial plantar branch is traced along the margin of the flexor sheath of the hallucis longus. The lateral branch is followed distally and the deep fascia of the abductor hallucis is released. Fibrous bands that are found to be constricting the nerves should be carefully released.
After the release, all the branches of the tibial nerve should be lying free. Haemostasis is carried out and a layered closure is performed.
Postoperative Care
A mild compression dressing is applied and the ankle is immobilized in slight inversion by using a splint for 3 weeks. After the splint is removed, the patient can begin joint mobilization.
Complications
Several complications of compression release surgery can arise. Most of the complications can be minimized with meticulous dissection.
Injury to the nerve or artery could have deleterious effects on foot function. Inadequate release of the retinaculum along its entire course may lead to poor postoperative outcome. This is the most likely cause of surgical failure.
A study by Kim and Dellon [26] showed that a neuroma of the distal saphenous nerve has to be considered as a causative factor if pain continues after surgical release.
Long-Term Monitoring
For proper healing to occur the patient should be nonweightbearing for a period of 3 weeks. Early mobilization is initiated to decrease the formation of scar tissue, which can contribute to compression neuropathy. Surgical shoe aids can be used to help reduce pressure on the surgical site. Physiotherapy can help the patient regain strength and motion and relief of residual pain.
After the removal of sutures, the patient should be able to resume the use of soft shoes. Shoes that can cause pressure and irritation of the surgical site should be avoided. In patients with pes planus, insole orthoses should be used to stabilize the medial column.
References
Alshami AM, Babri AS, Souvlis T, Coppieters MW. Biomechanical evaluation of two clinical tests for plantar heel pain: the dorsiflexion-eversion test for tarsal tunnel syndrome and the windlass test for plantar fasciitis. Foot Ankle Int. 2007 Apr. 28 (4):499-505.
Bracilovic A, Nihal A, Houston VL, Beattie AC, Rosenberg ZS, Trepman E. Effect of foot and ankle position on tarsal tunnel compartment volume. Foot Ankle Int. 2006 Jun. 27 (6):431-7.
DiDomenico LA, Masternick EB. Anterior tarsal tunnel syndrome. Clin Podiatr Med Surg. 2006 Jul. 23 (3):611-20.
Franson J, Baravarian B. Tarsal tunnel syndrome: a compression neuropathy involving four distinct tunnels. Clin Podiatr Med Surg. 2006 Jul. 23 (3):597-609.
Lamm BM, Paley D, Testani M, Herzenberg JE. Tarsal tunnel decompression in leg lengthening and deformity correction of the foot and ankle. J Foot Ankle Surg. 2007 May-Jun. 46 (3):201-6.
Vijayan J, Therimadasamy AK, Teoh HL, Chan YC, Wilder-Smith EP. Sonography as an aid to neurophysiological studies in diagnosing tarsal tunnel syndrome. Am J Phys Med Rehabil. 2009 Jun. 88 (6):500-1.
Dellon AL. The four medial ankle tunnels: a critical review of perceptions of tarsal tunnel syndrome and neuropathy. Neurosurg Clin N Am. 2008 Oct. 19 (4):629-48, vii.
Lambert A, Ben Salem D, Regis A, Soichot P, Ricolfi F. [Post-traumatic tarsal tunnel syndrome: interest of muscular MRI]. Rev Neurol (Paris). 2008 Jan. 164 (1):77-81.
Almeida DF, Scremin L, Zúniga SF, Oh SJ. Focal conduction block in a case of tarsal tunnel syndrome. Muscle Nerve. 2010 Sep. 42 (3):452-5.
Parkhurst DB, Saffarian MR, Andary MT, Fajardo RS, Knake JJ. Accessory Flexor Digitorum Longus Presenting as Tarsal Tunnel Syndrome: A Case Series. Clin J Sport Med. 2022 May 1. 32 (3):e316-e318.
Daniels TR, Lau JT, Hearn TC. The effects of foot position and load on tibial nerve tension. Foot Ankle Int. 1998 Feb. 19 (2):73-8.
Mann RA, DuVries HL, Inman VT, eds. Surgery of the Foot. 5th ed. St Louis, Mo: Mosby-Year Book; 1986. 205-7.
Gondring WH, Trepman E, Shields B. Tarsal tunnel syndrome: assessment of treatment outcome with an anatomic pain intensity scale. Foot Ankle Surg. 2009. 15 (3):133-8.
Antoniadis G, Scheglmann K. Posterior tarsal tunnel syndrome: diagnosis and treatment. Dtsch Arztebl Int. 2008 Nov. 105 (45): 776-81.
McSweeney SC, Cichero M. Tarsal tunnel syndrome-A narrative literature review. Foot (Edinb). 2015 Dec. 25 (4):244-50.
Yu X, Jiang Z, Pang L, Liu P. Surgical efficacy analysis of tarsal tunnel syndrome: a retrospective study of 107 patients. Cell Tissue Bank. 2021 Mar. 22 (1):115-122.
Lalevée M, Coillard JY, Gauthé R, Dechelotte B, Fantino O, Boublil D, et al. Tarsal Tunnel Syndrome: Outcome According to Etiology. J Foot Ankle Surg. 2022 May-Jun. 61 (3):583-589.
Duran-Stanton AM, Bui-Mansfield LT. Magnetic resonance diagnosis of tarsal tunnel syndrome due to flexor digitorum accessorius longus and peroneocalcaneus internus muscles. J Comput Assist Tomogr. 2010 Mar-Apr. 34 (2):270-2.
Fantino O, Bouysset M, Pialat JB. Can the axial cross-sectional area of the tibial nerve be used to diagnose tarsal tunnel syndrome? An ultrasonography study. Orthop Traumatol Surg Res. 2021 Oct. 107 (6):102630.
Rinkel WD, Castro Cabezas M, Birnie E, Coert JH. The natural history of tarsal tunnel syndrome in diabetic subjects. J Plast Reconstr Aesthet Surg. 2020 Aug. 73 (8):1482-1489.
Hudes K. Conservative management of a case of tarsal tunnel syndrome. J Can Chiropr Assoc. 2010 Jun. 54 (2):100-6.
Uemura T, Watanabe H, Yanai T, Kawano H, Yoshida A, Okutsu I. A Minimally Invasive Full Endoscopic Approach to Tibial Nerve Neurolysis in Diabetic Foot Neuropathy: An Alternative to Open Procedures. Plast Reconstr Surg. 2021 Sep 1. 148 (3):592-596.
Krishnan KG. Endoscopic decompression of the tarsal tunnel. Tech Foot Ankle Surg. 2010 Jun. 9 (2):52-7.
Iborra Marcos A, Villanueva Martinez M, Sanz-Ruiz P, Barrett SL, Zislis G. Ultrasound-Guided Proximal and Distal Tarsal Decompression: An Analysis of Pressures in the Tarsal, Medial Plantar, and Lateral Plantar Tunnels. Foot Ankle Spec. 2021 Apr. 14 (2):133-139.
Gültaç E, Kılınç B, Kılınç CY, Yücens M, Aydogan NH, Öznur A. Comparison of tunnel ligament release instrument assisted minimally open surgery and conventional open surgery in the treatment of tarsal tunnel syndrome. J Orthop Surg (Hong Kong). 2020 Sep-Dec. 28 (3):2309499020971868.
Kim J, Dellon AL. Pain at the site of tarsal tunnel incision due to neuroma of the posterior branch of the saphenous nerve. J Am Podiatr Med Assoc. 2001 Mar. 91 (3):109-13.