Management of Hand Extensor Tendon Injuries
Dr. KS Dhillon
Introduction
The extensor tendons function to transmit tension from the muscle belly to the specific joints of the hand. Extensor tendons are divided into two groups namely the intrinsic and extrinsic groups [1]. The intrinsic muscles are located within the hand itself. The extrinsic muscles are located proximally in the forearm and insert into the hand by long tendons [1]. The extensor muscles are all extrinsic except for the interosseous-lumbrical complex [1]. The lumbrical muscles produce flexion of the metacarpophalangeal (MP) joints and extension of the interphalangeal (IP) joints [1]. The interossei group forms the lateral bands with the lumbricals muscles and they adduct and abduct the fingers [1]. The radial nerve innervates all the extrinsic extensors. The extrinsic extensors consists of 3 wrist extensors as well as a larger group of thumb and digit extensors [1]. The extensor carpi radialis brevis (ERCB) is the main wrist extensor. Other extensors include extensor carp radialis longus (ECRL) and extensor carpi ulnaris (ECU) which also provide radial and ulnar movement of the wrist respectively [1]. The ECRB inserts at the base of the third metacarpal. The ECRL inserts at the base of the second metacarpal and the ECU at the base of the fifth metacarpal [2].
The extensor digitorum communis, extensor digiti minimi, and extensor indicis proprius extend the digits [2]. These muscles insert at the base of the middle phalanges as central slips and to the base of the distal phalanges as lateral slips [2]. Extension of the thumb is carried out by the extensor pollicus longus, abductor pollicis longus, and extensor pollicis [1]. There is an extensor retinaculum at the wrist which prevents bowstringing of the tendons at the wrist level and separates the tendons into 6 compartments [1]. The extensor digitorum muscle (also known as extensor digitorum communis) is a muscle of the posterior forearm. It extends the medial four digits of the hand. It is innervated by the posterior interosseous nerve, which is a branch of the radial nerve. The index and little fingers are also extended by the extensor indicis proprius and extensor digiti minimi [1]. The first extensor compartment of the wrist contains the extensor pollicis brevis and the abductor pollicis longus. The second contains the extensor carpi radialis longus and extensor carpi radialis brevis. The third, compartment contains the extensor pollicis longus; the fourth, the four tendons of the extensor digitorum communis plus the extensor indicis proprius; the fifth, the extensor digiti quinti; and the sixth, the extensor carpi ulnaris [1].
Extensor Tendon Injuries
Extensor tendon injuries are more common than flexor tendon injuries [3]. They are very common (61%) [4] since they are not protected as well as the flexor tendons due to their superficial location under the the skin. Extensor tendon injuries are known to cause serious functional impairment. They have, however, not received as much attention in the literature as flexor tendon injuries [5]. To repair the extensor tendons the surgeon needs the same skills as required for flexor tendon repair. It is not a simple challenge, which is a common misconception [6-8].
Lacerations of the extensor tendon can occur at any site. Extensor tendons are difficult for surgeons to repair because of their small size compared to the flexors and their lack of collagen-bundle linkage, which reduces the grip strength available for the suture material [9]. The flat tendon profile in zones I to IV increases the surface area between the repaired tendon and the adjacent tissue, particularly bone. This makes it susceptible to adhesion formation. Furthermore, the cross-section of the extensors changes from semicircular to bioconcave disk in zones I to IV making durable repair difficult because of the thin but broad characteristics of the tendon [10].
Clinical Presentation
A detailed history is essential. It is important to know the mechanism of injury, the position of the finger during the injury, age, occupation, and handedness of the patient. There are several reasons why the mechanism of injury is important. Most lacerations on the dorsum of the hand and fingers are clean. If there is any contamination wound debridement would be needed. History should elicit whether there was a human bit. The patient should also be asked about the presence of a foreign body in the wound.
Physical examination should include a systemic and in-depth examination of both hands. The site of the laceration and the inability to extend a joint distal to it indicates that the extensor tendon has been divided. If the extensor tendon is completely divided the finger would be resting in flexion.
When testing the function of the extensor muscle of the hand, the extension must be against resistance. Extension of the hand digits is performed by several muscles in the forearm that insert onto the digits. The extensor digiti minimi extends the fifth digit. It can be tested by asking the patient to lay the hand flat on a surface and hyperextension the fifth digit. The extensor digitorum tendons extend the 2nd to 5th digits. With the hand lying flat on a surface the tendon of each finger can be tested by having the patient hyperextend the digits against resistance. Extension of the second finger is also performed by extensor indicis. Extension of the first digit is controlled by two muscles i.e. the extensor pollicis longus and brevis. The path of these two tendons defines the anatomical snuffbox that contains the radial artery and the scaphoid bone. Extension of the thumb at the interphalangeal joint and the metacarpophalangeal joint can be tested separately.
Central slip injuries may not be immediately apparent on cursory examination after trauma. The Elson test can be useful in the identification of possible central slip injuries. The patient places the hand over the edge of a surface with the digits flexed at the proximal interphalangeal (PIP) joint and hanging freely. The examiner applies firm, constant pressure to the digit in question at the level of the middle phalanx. The patient then attempts to extend the finger at the PIP joint in opposition to the examiner’s applied force. If the patient is able to extend the PIP joint while the distal interphalangeal (DIP) joint remains pliable, it can be concluded that the central slip is intact. If there is an injury to the central slip, the patient will only be able to extend the PIP joint through the use of the lateral bands, which will lead to DIP joint rigidity and concomitant extension or even hyperextension at the DIP joint.
Sensation testing can be carried out to rule out radial nerve injury. The median and ulnar nerve should also be tested. Radiographs are done to assess any associated fracture that needs to be fixed before tendon and nerve injuries are treated. Human bites are also known to cause metacarpal fractures. Foreign objects including glass can be picked up on X-rays.
The extrinsic and intrinsic components of the extensor system can act independently. Hence full extension of the digits at the individual small joint of the hand is possible even after a laceration. The extension of the distal IP joint of the finger is still possible with complete severance of the main extrinsic extensor tendon at or proximal to the metacarpophalangeal joints. Furthermore, oblique retinacular ligaments can produce weak distal extension through the tenodesis effect.
The extensor mechanism usually fails at the insertion of the central slip and the terminal tendon producing characteristic deformities including the mallet and boutonniere deformity. In addition, mallet fingers can be complicated by extensor lag at the distal IP joint. A swan neck deformity can result as excess tension builds at the central slip insertion into the base of the middle phalanx.
Repair Of Extensor Inuries
Kleinert and Verdan [11] have created a classification system for extensor tendon lacerations according to the eight zones of the hand, wrist, and forearm. This classification has been widely accepted. Verdan defined eight zones (fig 1). Four odd-numbered zones overlie each of the joints and four even-numbered zones overlie the intervening tendon segments, increasing from distal to proximal. The type of injury, the surgical approach, and potential deformity vary according to the zone [11].
Zone I refers to the area from the DIP joint to the fingertip; zone II encompasses the middle phalanx; zone III refers to the PIP joint; zone IV is over the proximal phalanx; zone V refers to the MP joint; zone VI encompasses the metacarpal and zone VII is over the wrist [11].
According to Rockwell et al [12], the treatment of tendon injuries is dependent on the location and type of injury. Repair should be done very soon after the injury, especially within the first 2 weeks.
Extensor tendon repair techniques are not as complicated as flexor tendon repairs. This is because the extensor tendon is smaller with a relatively flat cross section. Its collagen is longitudinally orientated. There is little or no cross-linking. Due to the size differential and surrounding paratendon, except in zone VII, extensor tendons are not as capable of withstanding multiple-stranded, strong repair approaches, especially in the distal zones.
Unfortunately, there are very few studies that have investigated the strength of extensor repairs. The four-strand repair by Howard et al [13] has been shown to be the strongest. The biomechanical features including shortening, and loss of motion and strength were not evaluated in the study.
Compared with augmented Massachusetts General Hospital (MGH) Becker extensor tendon repair, or the traditional modified bunnel repair, two-strand locked bunnell repair has been found to be immediate in strength. It was evaluated further by Newport et al [14]. In these studies the locked bunnell improved the quality of strength over the traditional bunnell (17% versus 58% pullout) but less than the MGH repair (0% pullout) and the four-strand Bunnell or Kracjkow-Thomas (0% pullout) repair that was described by Howard et al [9].
The strength and the quality of the repair compared to the traditional two-stranded technique differs in the smaller, thinner tendons of zone IV as compared to repair in zone VI [9,15].
The tension strength of the extensor repair has not been studied in depth. Ketchum et al [15] investigated the tension strength via a force transducer on the proximal phalanx. They found that normal subjects could generate a force of 2.99 kg for the index finger. This decreased ulnarly to 1.97kg for the little finger. Studies in animal models have illustrated that tendon shortening can affect how the extensor tendon repair works by causing a loss of composite flexion and increasing the force required to obtain full flexion. Newport and Williams [9] showed that the modified bunnell technique can produce an average of at least 7mm of shortening resulting in 35 degrees or more loss of composite flexion when the wrist is held in a neutral position [9]. Minamikawa et al [16] also showed that there was a loss of 6.4 mm tendon over the metacarpal when the wrist was extended 45 degrees or more and they recommended that this could be amended if the wrist was appropriately extended. However, these are only animal studies so further research is still needed. The animal models cannot take into account muscle tone, adhesion formation, friction of edema, skin closure, or bulk of repair.
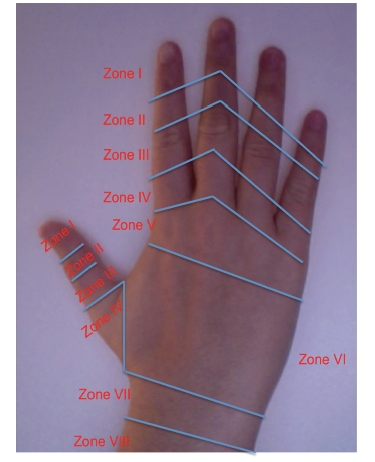
Fig 1.
Zone I Injuries
Zone I injury is referred to as a mallet finger. In this injury, there is disruption to the extensor tendon over the distal interphalangeal joint causing a flexion deformity of the distal interphalangeal joint [17]. It is usually a close injury but it can be open at times. The most likely cause is forceful flexion of the distal interphalangeal joint which is extended. This will result in a rupture of the extensor tendon or avulsion from its insertion at the distal phalanx. When it is left untreated hyperextension of the proximal interphalangeal joint may develop due to the retraction of the central band causing a swan neck deformity [18]. Mallet fingers are classified into 4 types:
Type 1: Close injury with or without avulsion fracture
Type 2: Laceration at or proximal to the distal interphalangeal joint with loss of tendon continuity
Type 3: Deep abrasion with loss of skin, subcutaneous tissue, and tendon substance
Type 4: (A) Transepiphyseal plate fracture in children; (B) hyperflexion injury with fracture of the articular surface of 20 to 50%; and (C) hyperextension injury with fracture of the articular surface greater than 50% and with early or late palmar subluxation of the distal phalanx.
Closed type I mallet injury is treated with an immobilization splint in extension or slight hyperextension for 8 weeks. This would include 2 weeks of night splinting. Exercises start by blocking exercises of the profundus involving the proximal interphalangeal joint active motion. A Cochrane review found that patient compliance was the most important factor in the success of splinting [19]. Another Cochrane review found that there was no evidence of difference in the outcomes between splints [20]. After 8 weeks the fingers should be reexamined to see if active extension is present. Splinting can now be reduced to high-risk times such as manual work, sleeping, or athletic performance. Splinting can be useful even after 3 months of the injury [21,22].
Type 2-4 injuries should be treated surgically. Type 2 requires a simple suture through the tendon alone or a roll-type suture incorporating the tendon and skin in the same suture and then splinting for 6-8 weeks [23]. Type 3 fractures include loss of tendon substance which requires immediate soft tissue coverage and primary grafting or reconstruction with a free tendon graft [23]. Type 4A injuries are best treated with closed reduction followed by splinting. These are the most likely fractures in children [23]. Type 4B injuries are usually treated by splinting for 6 weeks with 2 weeks of night splinting. This treatment yields good results. Type 4C with palmar subluxation of the distal phalanx is treated surgically with open reduction and internal fixation using a Kirschner wire and sometimes a pull-out wire or suture. A splint is used for 6 weeks. After 6 weeks the Kirschner wire is removed and motion started. The fracture fragment’s location is very important as proximally displaced fragments not in continuity with the distal phalanx may also require open reduction and internal fixation.
Chronic mallet finger is common. This is because some patients accept the deformity and never see a doctor for treatment. For those who present late splinting is the first line of treatment. Several reports have shown good outcome in patients who present late and are treated by splinting. Surgery is offered if conservative treatment fails or patients present with recurrent chronic mallet deformities. The treatment includes immobilization with transartilcular Kirschner wire fixation across the affected joint, fowler central slip release, excision of tendon scar, and fixation in hyperextension. Amputation and distal interphalangeal joint arthrodesis are the only two salvage procedures available [24-26].
Zone II injuries
Zone II injuries or middle phalanx injuries are usually due to a laceration or crush injury rather than avulsion as in zone I. If examination shows an extensor lag then exploration and repair is needed. If there is active extension with only a degree of weakness then splinting can be used for 3-4 weeks. Injuries with greater than 50% of the tendon torn or cut should be repaired. The tendon is repaired with a fashion-of-eight suture.
Zone III injuries
Zone III Injury produces a boutonniere deformity. It is caused by disruption of the central slip at the proximal interphalangeal joint. Examination shows absent or weak active extension of the proximal interphalangeal joint [27]. Active extension is initially retained by the lateral bands but the head of the proximal phalanx eventually goes through the central slip resulting in migration of the lateral bands. This then results in loss of extension at the proximal interphalangeal joint and hyperextension at the distal interphalangeal joint leading to boutonniere deformity. The injury can be open or close and the central slip can avulse with or without the bony fragment. The boutonniere deformity usually occurs 10-14 days after the initial injury [8]. Closed deformities require splinting for 4-6 weeks of the PIP joint in extension with the wrist joint and DIP joint left free. Surgery should be carried out for closed fractures when:
When there is a displaced avulsion fracture at the base of the middle phalanx
When there is axial and lateral instability of the PIP joint associated with loss of active or passive extension of the joint
When non-operative treatment fails.
During surgery, a suture is passed through the central tendon and secured to the middle phalanx with or without the bony fragment. Kirschner wire fixation of the proximal interphalangeal joint is maintained for 10 to 14 days. This is followed by an extension splint until union. If a primary repair is not possible then the lateral bands can be sutured in the dorsal midline of the finger to reconstruct the central slip. A flap can be raised from the proximal portion of the central slip to restore active extension. For open injuries, surgical repair is sometimes not required if splinting is used. However, in a true boutonniere deformity, both central slip and lateral band injuries can be expected. In the elderly, the period of immobilization can be reduced to 2 weeks to help in returning of full flexion.
Zone IV injuries
Zone IV injuries are proximal phalanx injuries. They usually involve the broad extensor mechanism. The injuries are usually partial and spare the lateral bands. They are usually diagnosed by inspection [28]. Splinting the PIP joint in extension for 3-4 weeks without repair has shown to have the same outcome as repairing it with 5 zero nonabsorbable sutures [29]. However, if the laceration is complete primary surgical repair has to be performed followed by 6 weeks of splinting in extension [30]. In the first 3 weeks, volar splinting is used with passive extension allowed. At week 4 gentle active extension is started but no passive flexion is allowed. In the last two weeks, active flexion is started, and graded resisted exercises are carried out.
Zone V injuries
Injuries in zone V are nearly always open. They are treated as human bites until examination proves otherwise. After wound irrigation primary tendon repair is required. The sagittal bands have to be repaired to prevent lateral migration of the extensor digtorum communis tendon and subsequent metacarpophalangeal extension loss [8,29].
After surgery, splinting of the wrist in 30-45 degrees of extension and the metacarpophalangeal joint in 20-30 degrees of flexion is done with the proximal interphalangeal joint free. If there is a human bite the wound should be extended for inspection and debrided, irrigated, and should be left open [30]. Cultures are taken before irrigation and patients are started on broad-spectrum antibiotics. The bite wound usually heals within 5 to 10 days. Secondary repair is rarely required.
Zone VI injuries
The tendons in this area are close to the thin subcutaneous tissue and thin paratendon. Injuries in this zone are situated in the dorsum of the hand. These injuries may not always result in loss of the extension at the MP joint. Surgical repair is done with stronger core-type sutures followed by splinting. The splinting should be placed in extension for 4-6 weeks. If the extensor digitorum communis is involved, all the fingers should be splinted. If the proprius tendon is solely involved, only the affected finger needs to be splinted with the wrist joint [31]. Degloving injuries that require grafting and flaps are not uncommon. Since the tendons in this area are larger, stronger core suture has to be used.
Zone VII injuries
There is still debate about releasing the retinaculum for visualization and repair of the tendon when injuries occur in this area. Such a release can produce postoperative adhesions [32,33]. Part of the extensor retinaculum has to be maintained to prevent tendon bowstringing [9]. With early dynamic splinting adhesions are less likely. A four-strand suture is appropriate for zone VII injuries.
Zone VIII injuries
Injuries to the dorsal forearm can produce laceration of many tendons, including the musculotendinous junction and tendon bellies. The thumb and wrist extensors should be repaired first [34]. Multiple figure of eight sutures are used to repair the muscle bellies. Static immobilization of the wrist in 45 degrees of extension and metacarpophalangeal joints in 15-20 degrees is maintained for 4-5 weeks [35].
Thumb injuries
Mallet injuries are uncommon in the thumb. This is because the terminal extensor tendon is thicker on the thumb [36]. For open injuries primary repair with splinting for 6 weeks is carried out. For closed injuries splinting for 6 weeks without surgical repair is a suitable alternative [37]. The broad expansion of the metacarpophalangeal joint of the thumb makes laceration of all components in this area uncommon. Extensor pollicis brevis is rarely lacerated in isolation. Its repair is debatable because extension of the metacarpophalangeal joint is possible with an intact extensor pollicis longus. Extensor pollicis longus injury causes extension lag in both metacarpophalangeal and interphalangeal joints. It has to be repaired. Splinting is done for 3 to 4 weeks, with the thumb metacarpophalangeal joint in full extension and the wrist in 40 degrees of extension with slight radial deviation. For injuries in zones VI and VII, the abductor pollicis longus retracts when divided. It has to be released for successful repair [28]. Splinting is done for 4-5 weeks with the wrist in radial deviation and the thumb in maximal abduction [28].
Rehabilitation of Extensor Injuries
The aim of rehabilitation is to obtain healing with minimal gapping in the tendon and to prevent adhesions. Static mobilisation has been the traditional method of postoperative rehabilitation. There can be several complications including tendon rupture, adhesion formation requiring tenolysis, extension lag, loss of flexion, and decreased grip strength [32,38-40].
Early mobilization was introduced for flexor tendon injuries to decrease adhesions and subsequent contractures. Mobilization has been shown to enhance DNA synthesis at the repair site, improve tensile strength, and increase the vascularity [41-43]. Now it has been shown to be more useful in certain areas for extensor injuries as well [44].
Mowlavi et al [45] studied early controlled mobilization versus static splinting for zone V and zone VI injuries [45]. They found that functional outcomes at 4,6 and 8 weeks were better after early controlled mobilization compared to static splinting [45]. However, the outcomes were not improved after 6 months [45]. The authors were of the opinion that dynamic splinting should be available to those who are motivated to return early to functional capacity.
Bulstrode et al [46] also found that ROM for the early mobilization group at 6 weeks postoperatively was greater than the static mobilization group but the differences disappeared at 12 weeks. The grip strength was also assessed at 12 weeks postoperatively [46]. They found that the difference in grip strength was significantly greater in the early-mobilized group compared to the immobilized [46].
Russell et al [47] also compared immobilization with early controlled mobilization but they found no significant difference in hand function between the groups.
Early mobilization rehabilitation programs can be of 2 types.
(1) early active mobilisation
(2) early controlled mobilization using a dynamic splint.
Early controlled motion with a dynamic extensor splint has been found to reduce adhesions and contractures. There are only two randomized controlled trial studies that have compared early mobilization versus early active mobilization. Chester et al [48] studied extensor injuries from zone IV to VIII and found significantly better ROM in the patient group treated with early controlled mobilization as compared to early active mobilization at 4 weeks. Khandwala et al [49] compared early active mobilization with early controlled mobilization in zones V and VI and they found no difference in total active motion at 4 or 8 weeks postoperatively. There are only a few studies that have tried to evaluate the specific mobilization regime that has the best functional outcome.
A recent review by Talsmaby et al [50] confirmed that short-term evidence shows early controlled mobilization is superior over immobilization for extensor tendons. There is no conclusive evidence regarding the long-term effectiveness of the different rehabilitation programs. In addition, the study highlighted that there is a wide variety in the duration of splinting, splinting technique, and frequency and force intensity of exercises used for rehabilitation. Evaluation of the cost-effectiveness of the treatment regimes' showed that dynamic splinting is more expensive and requires more hand therapist input. This is why some authors prefer early active mobilization for proximal zone injuries [51,52].
Complications
Complications can occur after extensor tendon repair. These include loss of flexion due to extensor tendon shortening, loss of flexion and extension due to adhesions, and a weak grip. When the extensor tendon becomes shortened or adherent, tenodesis restraint occurs. Flexion of the digit at the MP joint causes extension force at the PIP joint. Hand therapy has to be started and it should focus on extrinsic excursion exercises. Splinting should be started immediately.
If there is no improvement following 6 months of conservative treatment then surgery may be needed. Tenolysis is appropriate when tenodesis occurs as a result of scarring with no significant loss of tendon length. If the tendon is shortened, Littler’s technique of extensor tendon release can be used [53]. Eggli et al [54] evaluated the clinical outcomes in 23 patients after tenolysis and they found that on average follow-up of 5 years, significant improvement occurred in 88% of the digits in extensor and flexor injuries in zone II. Extensor tenolysis was also found to be a safe procedure [54].
In Zone VII and VIII injuries, there can be multiple tendon lacerations. These injuries can lead to decreased wrist mobility. Human bite injuries in zone V can be complicated by infection. Zone I, II and III injuries can be complicated by deformities. Newport et al [32] retrospectively reviewed 62 patients with 101 extensor tendon injuries and they found that patients without associated injuries achieved 64% good to excellent results and total active motion of 212 degrees which was statistically significant. Distal zones (I to IV) had poorer outcomes as compared to proximal zones (V to VIII). The percentage of fingers losing flexion was greater than those losing extension. This study showed that the loss of flexion was a more significant complication of extensor tendon injuries.
Staged extension tendon repair can be carried out after failed primary repair. It involves tendon reconstruction using a silicone implant. Small skin incisions are made over the dorsum of the finger and a silicone rod is placed along the pretendious fascia to create a tunnel. Soft tissue defects are treated by split-thickness skin grafts or by secondary suture. Once the wounds have healed, the silicone rod is exchanged for a tendon graft. Adams [55] used this technique in 6 fingers to restore proximal joint extension in patients with severe injuries to the dorsal skin and extensor mechanism. He restored active extension of all proximal interphalangeal joints. He recommended it as a reliable alternative for severely injured fingers with extensor mechanism loss.
Conclusion
The literature has not focused on extensor tendon injuries to the same extent as flexor tendon injuries. Rehabilitation methods have been researched and it is clear that mobilization techniques are more favored. The surgical approach to each zone has not been fully researched. There are very few papers looking at the outcomes of different approaches. More research is needed to work out the optimal approach to extensor tendon injuries and to study the complication rates after different approaches.
References
Moore KL, Dalley AF. Clinically orientated anatomy. 5th. Baltimore: Lippincott Williams and Wilkins; 2005.
Drake R, Vogl W, Mitchell A. Grays Anatomy for students. 1st. London: Churchill Livingstone; 2004.
Tuncali D, Yavuz N, Terzioglu A, Aslan G. The rate of upper-extremity deep-structure injuries through small penetrating lacerations. Ann Plast Surg. 2005;55:146–8.
Hague MF. The results of tendon suture of the hand: a review of 500 patients. Acta Orthop Scand. 1954;24:258.
Crosby CA, Wehbé MA. Early protected motion after extensor tendon repair. J Hand Surg. 1999;24:1061–70.
Kelly AP., Jr Primary tendon repair: a study of 789 consecutive tendon severances. J Bone Joint Surg Am. 1956;41:581–98.
Zander CL. The use of early mobilization following complex injury to the extensor tendons. J Hand Ther. 1987;1:38–41.
Hart RG, Uehara DT, Kutz JE. Extensor tendon injuries of the hand. Emerg Med Clin North Am. 1993;11:637.
Newport ML, Williams CD. Biomechanical characteristics of extensor tendon suture techniques. J Hand Surg. 1992;17A:1117–23.
Woo SH, Tsai TM, Kleinert HE, Chew WY, Voor MJ. A biomechanical comparison of four extensor tendon repair techniques in zone IV. Plast Reconstr Surg. 2005;115:674–81.
Kleinert HE, Verdan C. Report of the committee on tendon injuries. J Hand Surg. 1983;8:794.
Rockwell WB, Butler PN, Byrne BA. Extensor tendon: Anatomy, injury, and reconstruction. Plast Reconstr Surg. 2000;106:1592.
Howard RF, Ondrovic L, Greenwald DP. Biomechanical analysis of four-strand extensor tendon repair techniques. J Hand Surg Am. 1997;22(5):838–42.
Newport ML, Pollack GR, Williams CD. Biomechanical characteristics of suture techniques in extensor zone IV. J Hand Surg Am. 1995;20:650–6.
Ketchum LD, Thompson D, Pocock G, Wallingford D. A clinical study of forces generated by the intrinsic muscles of the index finger and the extrinsic muscles of the hand. J Hand Surg. 1978;6:571–8.
Minamikawa Peimer CA, Yamaguchi T, Banasiak NA, Kambe K, Sherwin FS. Wrist position and extensor tendon amplitude following repair. J Hand Surg Am. 1992;17:268–71.
Anderson D. Mallet finger - management and patient compliance. Aust Fam Physician. 2011;40(1-2):47–8.
Evance D, Weightman B. The pipeflex splint for treatment of mallet finger. J Hand Surg Br. 1988;13:156.
Handoll HH, Vaghela MV. Interventions for treating mallet finger injuries. Cochrane Database Syst Rev. 2004;3:cD004574.
Handoll HH, Vaghela MV. Interventions for treating mallet finger injuries (review) Cochrane Database Syst Rev. 2008;3 Art no. cD004574.
Palmer Re. Joint injuries of the hand in athletes. Clin Sport Med. 1998;17:513–31.
Garberman SF, Diao E, Peimer CA. Mallet finger: results of early versus delayed closed treatment. J Hand Surg. 1994;19A:850–2.
Doyle JR. Extensor tendons: acute injuries. In: Green DP, editor. Operative Hand Surgery. 3rd. New York: Churchill Livingstone; 1993. pp. 1925–51.
Abouna JM, Brown H. The treatment of mallet finger. Br J Sur. 1968;55:653.
Garberman S, Diao FE, Peimer CA. Mallet finger: results of early versus delayed closed treatment. J Hand Surg Am. 1994;19:850.
Patel MR, Desai S, Bassini-Lipson L. Conservative management of chronic mallet finger. J Hand Surg Am. 1986;11:570.
Elson RA. Rupture of the central slip of the extensor hood of the finger: a test for diagnosis. J Bone Joint Surg Br. 1986;68:229.
Verdan CE. Primary and Secondary Repair of Flexor and Extensor Tendon Injuries. In: Flynn JE, editor. Hand Surgery. 2nd ed. Baltimore: Williams & Wilkins; 1975.
Blair WF, Steyers CM. Extensor tendon injuries. Orthop Clin North Am. 1992;23:141.
El-Gammal TA, Steyers CM, Blair WF, Maynard JA, Chapman MW. Anatomy of the oblique retinacular ligament of the index finger. J Hand Surg Am. 1993;18:717.
Thompson JS, Peimer CA. Extensor Tendon Injuries: acute repair and late reconstruction. In: Chapman MW, editor. Operative Orthopaedics. Philadelphia: Lippincott; 1998.
Newport ML, Blair WF, Steyers CM. Long- term results of extensor tendon repair. J Hand Surg Am. 1990;15:961.
Browne EZ, Jr, Ribik CA. Early dynamic splinting for extensor tendon injuries. J Hand Surg Am. 1989;14:72.
Willson RL. Management of Acute Extensor Tendon Injuries. In: Hunter JM, Schneider LH, Mackin EJ, editors. Tendon Surgery in the Hand. St. Louis: Mosby; 1987.
El-Gammal TA, Steyers CM, Blair WF, Maynard JA. Anatomy of the oblique retinacular ligament of the index finger. J Hand Surg Am. 1993;18:717.
Patel MR, Lipson L-B, Desai SS. Conservative treatment of mallet thumb. J Hand Surg Am. 1986;11:45.
Din KM, Meggitt BF. Mallet thumb. J Bone Joint Surg Br. 1983;65:606.
Browne EZ, Jr, Ribik CA. Early dynamic splinting for extensor tendon injuries. J Hand Surg Am. 1989;14:72–6.
Bruner S, Wittemann M, Jester A, Blumental K, Germann G. Dynamic splinting after extensor repair in zones V to VII. J Hand Surg. 2003;28(3):224–7.
Evans RB, Burkhalter WE. A study of the dynamic anatomy of extensor tendons and implications for treatment. J Hand Surg Am. 1986;1:74–9.
Newport ML, Tucker RL. New perspectives on extensor tendon repair and implications for rehabilitation. J Hand Ther. 2005; 18:175–81.
Hitchcock TF, Light TR, Bunch WH, Knight GW, Sartori MJ, Patwardhan AG. The effect of immediate constrained digital motion on the strength of flexor tendon repairs in chickens. J Hand Surg. 1987;12A:590–5.
Feehan LM, Beauchene JG. Early tensile properties of healing chicken flexor tendons: early controlled passive motion versus postoperative immobilization. J Hand Surg. 1990;15A:63–8.
Evans RB. Therapeutic management of extensor tendon injuries. Hand Clin. 1986;2:157–6.
Mowlavi A, Burns M, Brown RE. Dynamic versus static splinting of simple zone V and zone VI extensor tendon repairs: a prospective, randomized, controlled study. Plast Reconstr Surg. 2005;115:482–7.
Bulstrode NW, Burr N, Pratt AL, Grobbelaar AO. Extensor tendon rehabilitation a prospective trial comparing three rehabilitation regimes. J Hand Surg Br. 2005;30:175–9.
Russell RC, Jones M, Grobbelaar A. Extensor tendon repair: mobilise or splint? Chir Main. 2003;22:19–23.
Chester DL, Beale S, Beveridge L, Nancarrow JD, Titley OG. A prospective, controlled, randomized trial comparing early active extension with passive extension using a dynamic splint in the rehabilitation of repaired extensor tendons. J Hand Surg Br. 2002;27:283–8.
Khandwala AR, Webb J, Harris SB, Foster AJ, Elliot D. A comparison of dynamic extension splinting and controlled active mobilization of complete divisions of extensor tendons in zones 5 and 6. J Hand Surg Br. 2000;25:140–6.
Talsma E, de Haart M, Beelen A, Nollet F. The effect of mobilization on repaired extensor tendon injuries of the hand: a systematic review. Arch Phys Med Rehabil. 2008;89(12):2366–72.
Bulstrode NW, Burr N, Pratt AL, Grobbelaar AO. Extensor tendon rehabilitation a prospective trial comparing three rehabilitation regimes. J Hand Surg. 2005;30B:175–9.
Khandwala AR, Webb J, Harris SB, Foster AJ, Elliot D. A comparison of dynamic extension splinting and controlled active mobilization of complete divisions of extensor tendons in zones 5 and 6. J Hand Surg. 2000;25B:140–6.
Littler JW. The finger extensor mechanism. Surg Clin North Am. 1967;47:415.
Eggli S, Dietsche A, Vogelin E. Tenolysis in combined digital injuries in zone II. Ann Plast Surg. 2005;55:266–71.
Adams BD. Staged extensor tendon reconstruction in the finger. J Hand Surg Am. 1997;22(5):833–7.