Chopart injuries
Dr. KS Dhillon
Introduction
The transverse-tarsal or midtarsal joint is known eponymously as the Chopart joint after French surgeon François Chopart. He described an amputation through the articulation between the hindfoot and the midfoot(1). The Chopart joint is made up of the talonavicular joint (TNJ) and calcaneocuboid joint (CCJ). The TNJ is part of the coxa pedis (talocalcaneonavicular joint) which enables supination and pronation of the tarsus (2). The CCJ provides approximately 25° of rotation for hindfoot inversion and eversion (3). The Chopart joint complex allows the hindfoot to pivot while the forefoot remains still with inversion and eversion. The complex locks on heel inversion, stabilizing the midfoot during the push-off phase of gait (4). The Chopart joint is essential for normal foot function and requires strong ligamentous support. The TNJ is bridged superiorly by the dorsal talonavicular ligament and medial limb of the bifurcate ligament and inferiorly by the spring ligament (calcaenonavicular ligament). The spring ligament is comprised of the medioplantar oblique, inferoplantar longitudinal, and superomedial components (4) (fig 1).
Superiorly the CCJ is supported by the dorsal calcaneocuboid ligament and the lateral limb of the bifurcate ligament and inferiorly by the short plantar ligament (plantar calcaneocuboid ligament) (4).
The cyma line divides the midfoot and the hindfoot. It represents the Chopart joint. It can be observed via dorsoplantar and lateral views (5), where radiological discrepancy indicates pathology. Initial imaging starts with radiographs in 3 views: dorsoplantar, lateral, and oblique (6). Oblique views are best for visualizing fractures of the anterior calcaneal process (4).
The Chopart injuries can be divided into 4 broad groups:
Ligamentous injury with dislocation
Ligamentous injury without dislocation
Fracture with dislocation
Fracture without dislocation.
Chopart dislocations can be pure-dislocations and fracture-dislocations.
Pure dislocations are dislocations of the navicular and/or cuboid without an associated fracture. Fracture-dislocations are dislocations of the navicular and/or cuboid with associated fracture of the talus, navicular, calcaneus, or cuboid bones. Simultaneous dislocation of both the CCJ and TNJ is referred to as a complete Chopart dislocation. Swivel dislocations usually result from medial or lateral deforming forces causing CCJ and/or TNJ dislocation and the calcaneus ‘swivels’ on an intact talocalcaneal ligament (7).
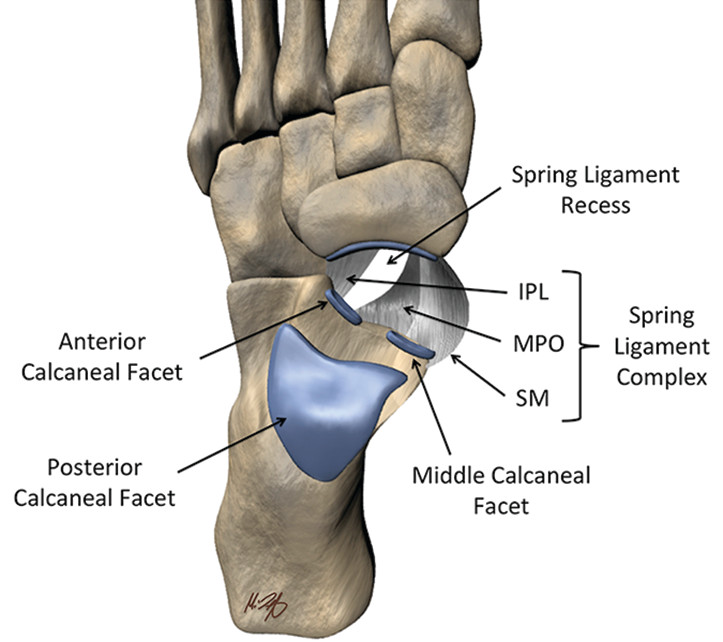
Fig 1.
Incidence and etiology
Ponkilainen et al (8) conducted a retrospective epidemiology cohort study of 307 midfoot injuries. They found that the incidence of midfoot injury is 12.1/100,000/year and Chopart injury 2.2/100,000/year. Motor vehicle accidents (MVA) are the main cause of Chopart dislocations. Chopart dislocations are more common in males (6,9). Richter et al. found that 16% of 155 midfoot fractures were Chopart fracture-dislocations(9). Richter et al in a follow-up study of 110 Chopart-dislocations found that 25% were pure-dislocations, 55% fracture-dislocations, and 20% combined Chopart-Lisfranc fracture-dislocations (6). A recent study by Rammelt et al (10) of 128 Chopart joint injuries found only 5 patients (3.7%) had pure-dislocations and the most frequent fracture-dislocation was transnavicular/transcuboidal in 21% of cases. The average age of patients in 5 studies was 36.8 years (11).
Diagnosis
Chopart injuries are clinically diagnosed through a careful history and physical examination. Radiographic evaluation is required to exclude fractures or assess syndesmotic integrity.
Clinical signs
Clinical examination will show plantar ecchymosis. Plantar ecchymosis sign (PES) describes a central midfoot plantar ecchymosis that is pathognomic for relevant midfoot injuries. It indicates the rupture of strong plantar ligaments and resulting haematoma (12). PES has been seen following calcaneal fractures (13), Lisfranc (14), and Chopart injuries (15). The PES is rarely reported although it is a valuable clinical sign indicating underlying midfoot injury. A CT is useful when PES is positive and radiographs are negative. Compartment syndrome is common in Chopart injuries (9,10), especially dislocations (6). Palpation of the entire foot is necessary and conformation of the neurovascular statues is required.
Imaging
Up to 41% of Chopart injuries are missed at first presentation (5). Haapamaki et al (16) found that plain radiographs alone missed 33% of fractures in Chopart injuries. In Van Dorp et al (5) case series of 9 Chopart dislocations, 2 were initially missed from Xray alone and the severity of the injury was underestimated for 3 prior to CT. Alongside this 2/24 fracture-dislocations from case reports were initially missed on Xrays. Rammelt et al found pure-dislocations to be very rare (4%). They encourage CT scanning to rule out associated fractures (10). Almeida et al (17) also found a significant improvement in identifying additional Chopart fractures missed on XR with CT. CT allows reconstructive modelling to determine the degree of dislocation (4).
Management and outcomes
For Chopart dislocations, initial ORIF provides better outcomes than closed reduction prior to internal fixation (6). A study by Richter et al (6) found that a closed reduction can yield good results only with pure dislocations, when anatomic conditions can be restored, or if there were contraindications to surgery. Closed reduction alone was found to have statistically similar outcomes to operative treatment. Six of fourteen pure-dislocations required internal fixation following closed reduction and they should have undergone ORIF initially. Since there is a risk of requiring internal fixation following closed reduction, ORIF is advised and closed reduction is discouraged.
Closed reduction is often challenging. It often fails and repeated attempts can cause further damage (18). Rammelt et al (10) found over a 10-year follow-up that ORIF generates significantly better results than closed reduction and percutaneous fixation in patients with Chopart injuries. According to Rammelt et al (10), pure-dislocations had the worst prognosis.
Maintenance of foot column length is important. It significantly improves the gait quality (19). Correct alignment of the foot axes and correct length of medial and lateral columns should be a major goal of therapy (5).
Secondary reconstruction improves outcomes in suitable patients with malunited Chopart fracture dislocations. Otherwise, joint fusion is required (20). Arthrodesis is carried out in patients who present late (21), in patients with diabetic arthropathy (22), or when other treatment strategies have failed. Arthrodesis can prevent midfoot collapse (23). TNJ arthrodesis can reduce the Chopart joint range of motion by 50%. It is a negative prognostic factor (10). It is considered as a last resort (24). Soft tissue conditions dictate treatment methods. External fixation can maintain reduction during soft tissue healing (10,25). It also maintains column length with unstable ORIF (26). Patients with Chopart injuries require long-term follow-up to monitor for complications which are common (5,27).
Conclusion
Pure dislocations tend to have inferior outcomes. It is probably due to the high energy required to disrupt the strong ligamentous anatomy at the Chopart joint. A general consensus is that closed reduction often fails and leads to poorer outcomes, even if followed by ORIF. Restoring and maintaining the medial and lateral foot columns by joint reconstruction is essential to obtain satisfactory results. Compartment syndrome evaluation and CT are highly recommended. Urgent ORIF with or without external fixation is the management of choice for these injuries. Negative prognostic factors include the severity of injury, delayed or staged treatment, arthrodesis, and MVA.
References
Wolf JH. Francois Chopart (1743–1795) – inventor of the partial foot amputation at the transtarsal articulation. Orthop Traumatol. 2000;8(4):314–317.
Kou JX, Fortin PT. Commonly missed peritalar injuries. J Am Acad Orthop Surg. 2009;17(12):775–786. doi: 10.5435/00124635-200912000-00006.
Walter WR, Hirschmann A, Alaia EF, Tafur M, Rosenberg ZS. Normal anatomy and traumatic injury of the midtarsal (Chopart) joint complex: an imaging primer. Radiographics. 2019;39(1):136–152. doi: 10.1148/rg.2019180102.
Walter WR, Hirschmann A, Tafur M, Rosenberg ZS. Imaging of Chopart (midtarsal) joint complex: normal anatomy and posttraumatic findings. AJR Am J Roentgenol. 2018;211(2):416–425. doi: 10.2214/AJR.17.19310.
Van Dorp KB, de Vries MR, van der Elst M, Schepers T. Chopart joint injury: a study of outcome and morbidity. J Foot Ankle Surg. 2010;49(6):541–545. doi: 10.1053/j.jfas.2010.08.005.
Richter M, Thermann H, Huefner T, Schmidt U, Goesling T, Krettek C. Chopart joint fracture-dislocation: initial open reduction provides better outcome than closed reduction. Foot Ankle Int. 2004;25(5):340–348. doi: 10.1177/107110070402500512.
Pillai A, Chakrabarti D, Hadidi M. Lateral swivel dislocation of the talo-navicular joint. Foot Ankle Surg. 2006;12:39–41.
Ponkilainen VT, Laine HJ, Mäenpää HM, Mattila VM, Haapasalo HH. Incidence and characteristics of midfoot injuries. Foot Ankle Int. 2019;40(1):105–112. doi: 10.1177/1071100718799741.
Richter M, Wippermann B, Krettek C, Schratt HE, Hufner T, Therman H. Fractures and fracture dislocations of the midfoot: occurrence, causes and long-term results. Foot Ankle Int. 2001;22(5):392–398. doi: 10.1177/107110070102200506.
Rammelt S, Missbach T. Chopart joint injuries: assessment, treatment, and 10-year results. J Orthop Trauma. 2023;37(1):e14–e21. doi: 10.1097/BOT.0000000000002465.
Metcalfe TSN, Aamir J, Mason LW. Chopart dislocations: a review of diagnosis, treatment and outcomes. Arch Orthop Trauma Surg. 2024 Jan;144(1):131-147. doi: 10.1007/s00402-023-05040-4. Epub 2023 Sep 15. PMID: 37715068; PMCID: PMC10774188.
Rammelt S. Chopart and lisfranc fracture-dislocations. In: Bentley G, editor. European surgical orthopaedics and traumatology: the EFORT textbook. Berlin, Heidelberg: Springer Berlin Heidelberg; 2014. pp. 3835–3857.
Richman JD, Barre PS. The plantar ecchymosis sign in fractures of the calcaneus. Clin Orthop Relat Res. 1986;207:122–125.
Ross G, Cronin R, Hauzenblas J, Juliano P. Plantar ecchymosis sign: a clinical aid to diagnosis of occult Lisfranc tarsometatarsal injuries. J Orthop Trauma. 1996;10(2):119–122. doi: 10.1097/00005131-199602000-00008.
Dewar FP, Evans DC. Occult fracture-subluxation of the midtarsal joint. J Bone Joint Surg Br. 1968;50(2):386–388.
Haapamaki VV, Kiuru MJ, Koskinen SK. Ankle and foot injuries: analysis of MDCT findings. AJR. 2004;183:615–622. doi: 10.2214/ajr.183.3.1830615.
Almeida RR, Mansouri M, Tso DK, Johnson AH, Lev MH, Singh AK, Flores EJ. The added value of cross-sectional imaging in the detection of additional radiographically occult fractures in the setting of a Chopart fracture. Emerg Radiol. 2018;25(5):513–520. doi: 10.1007/s10140-018-1615-x.
Honeycutt MW, Perry MD. The Chopart variant dislocation: plantar dislocation of the cuboid and navicular. Foot Ankle Orthop. 2019;4(3):2473011419876262. doi: 10.1177/2473011419876262.
Mittlmeier T, Krowiorsch R, Brosinger S, Hudde M. Gait function after fracture-dislocation of the midtarsal and/or tarsometatarsal joints. Clin Biomech (Bristol, Avon) 1997;12(3): S16–S17. doi: 10.1016/s0268-0033(97)88330-1.
Rammelt S, Zwipp H, Schneiders W, Heineck J. Anatomic reconstruction of malunited Chopart joint injuries. Eur J Trauma Emerg Surg. 2010;36(3):196–205. doi: 10.1007/s00068-010-1036-3.
Kumar A, Gaba S, Digge VK, Gautam D. Neglected medial swivel talonavicular dislocation treated with arthrodesis: a case report and literature review. J Clin Orthop Trauma. 2020;11(3):474–478. doi: 10.1016/j.jcot.2018.12.011.
Ansari MAQ. Isolated complete dislocation of the tarsal navicular without fracture: a rare injury. Ci Ji Yi Xue Za Zhi. 2016;28(3):128–131. doi: 10.1016/j.tcmj.2014.11.003.
Arain AR, Adams CT, Haddad SF, Moral M, Young J, Desai K, Rosenbaum AJ. Diagnosis and treatment of peritalar injuries in the acute trauma setting: a review of the literature. Adv Orthop. 2020;2020:1852025. doi: 10.1155/2020/1852025.
Johnstone AJ, Maffulli N. Primary fusion of the talonavicular joint after fracture dislocation of the navicular bone. J Trauma. 1998;45(6):1100–1102. doi: 10.1097/00005373-199812000-00025.
Klaue K. Treatment of Chopart fracture-dislocations. Eur J Trauma Emerg Surg. 2010;36(3):191–195. doi: 10.1007/s00068-010-1047-0.
Kutaish H, Stern R, Drittenbass L, Assal M. Injuries to the Chopart joint complex: a current review. Eur J Orthop Surg Traumatol. 2017;27(4):425–431. doi: 10.1007/s00590-017-1958-0.
Kösters C, Bockholt S, Müller C, Winter C, Rosenbaum D, Raschke MJ, Ochman S. Comparing the outcomes between Chopart, Lisfranc and multiple metatarsal shaft fractures. Arch Orthop Trauma Surg. 2014;134(10):1397–1404. doi: 10.1007/s00402-014-2059-8.