Scaphoid fractures
Dr KS Dhillon
Scaphoid Bone Anatomy
The scaphoid is one of the carpal bones of the wrist (Fig 1). It lies in the proximal row of carpal bones on the lateral side of the wrist. The scaphoid bone is the largest bone of the proximal row of carpal bones. It is approximately the same shape and size of a medium-sized cashew. It is also known as os scaphoideum. It is important for stability and movements at the wrist joint.
The bone has a tubercle on its lateral side directed laterally, forwards and downwards. The superior surface is convex, smooth, triangular in shape, and articulates with the lower end of the radius. The inferior surface is directed downward, laterally, and backward. It is smooth, convex, and triangular, and is divided by a slight ridge into two parts, the lateral articulating with the trapezium, the medial articulating with the trapezoid.
On the dorsal surface there is a narrow, rough groove that runs the entire length of the bone, and gives attachment to ligaments.
The volar surface is concave above and has a tubercle that is directed forward and gives attachment to the transverse carpal ligament and sometimes gives origin to a few fibers of the abductor pollicis brevis muscle.
The lateral surface is narrow and rough and gives attachment to the radial collateral ligament of the wrist.
On the medial surface there are two articular facets. The superior articulates with the lunate bone and the inferior articulates with the head of the capitate bone. The distal convex surface articulates with trapezium and trapezoid.
The scaphoid articulates with five bones: the radius, trapezoid, trapezium, lunate and capitate. Proximally it articulates with the radius. On the distal surface it articulates laterally with the trapezoid and trapezium and medially with the capitate bone and the lunate.
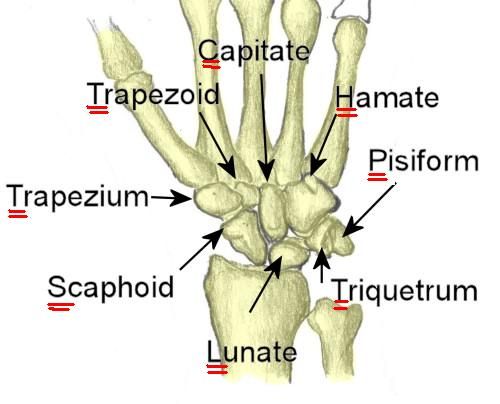
Fig 1- Carpal Bones
There are 5 ligaments attached to the scaphoid:
Dorsal radiocarpal ligament
Radial collateral ligament
Scapholunate ligament
Radioscapholunate ligament
Scaphocapitate ligament
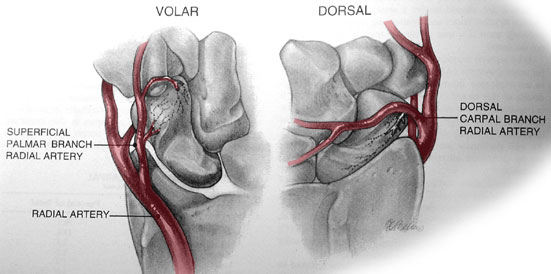
Fig 2- Blood supply to the scaphoid
The scaphoid receives most of its blood supply via dorsal vessels at or just distal to waist area passing through perforations on the dorsal surface. About 75% of the arterial supply is from branches of the radial artery. The rest of the blood supply comes from palmar & superficial palmar branches of the radial artery and enter the carpal scaphoid in the region of its distal tubercle perfusing 20-30 % of bone, including the tuberosity.
No anastomoses have been found between the dorsal and palmar vessels. The vascular supply to the proximal pole is mainly retrograde.
Fracture of the carpal scaphoid
Fractures of the scaphoid occur more often than fractures of other carpal bones. They account for 2% to 7% of all fractures and 60% to 70% of carpal bone fractures [1]. Scaphoid fractures account for 15% of acute wrist injuries.
Scaphoid fractures predominantly occur in young adults, with a mean age of 29 years [2]. The incidence is higher in males. Scaphoid fractures are uncommon in children and in the elderly individual. Scaphoid fractures account for 15% of acute wrist injuries.
Patients usually present with wrist pain following a fall on an outstretched hand. Axial loading of the wrist occurs with hyperextension and radial deviation. Such forces cause impaction of the scaphoid on the dorsal rim of the radius leading to a fracture.
About 65% of scaphoid fractures occur at the waist, with a quarter at the proximal third and 10% at the distal third of the scaphoid bone. There is strong association between the location of the fracture and incidence of avascular necrosis (AVN). Fractures in the proximal segment have a 100% rate of AVN, reducing to 33% for fractures at the distal segment of the scaphoid.
Patients usually present with pain and swelling at the base of the thumb in the anatomic snuffbox after a fall or wrist trauma. Pain is often on the radial side of the wrist and is worse with wrist movements. There may be associated swelling with a reduced range of wrist movements.
Tenderness is usually present in one of these three locations:
- On the volar prominence at the distal wrist for distal pole fractures
- On the anatomic snuffbox for waist fractures
- Distal to Lister's tubercle for proximal pole fractures
The scaphoid compression test will be positive. It is performed by placing the examining index finger and thumb over each pole of the scaphoid and compressing. Pain in the anatomical snuffbox on ulnar deviation of the wrist is also suggestive of a scaphoid fracture.
Diagnosis is confirmed with scaphoid AP view and lateral view x rays of the wrist. About 25% of scaphoid fractures are not evident on initial plain Xrays. If high clinical suspicion exists, the wrist should undergo immobilization in a splint or cast for 7-14 days and plain radiographs repeated. If early confirmation is needed, bone scans can be done to diagnose occult fractures at 72 hours post-injury.
When the clinical suspicion is high and the x-rays are normal, Magnetic Resonance Imaging (MRI) or Computed Tomography (CT) can be carried out [3]. MRI is the most sensitive means of diagnosing scaphoid fractures. MRI can also identify any associated ligamentous injury or bone edema [4]. A meta-analysis by Yin et al [5] estimated 97.7% sensitivity and 99.8% specificity with an MRI. Although CT scan has high sensitivity and specificity, fractures with less than 1 mm displacement can be missed.
Treatment of scaphoid fractures
Scaphoid fractures can be treated surgically or conservatively.
Nonoperative Management
Fractures that are undisplaced and in the distal third of the bone can be managed non-operatively with cast immobilization [6]. There is presently no consensus as to whether a long or short arm cast is optimal and whether a thumb spica should be included to immobilize the thumb.
The cast is usually required for six weeks and repeat x-rays are taken at this time to assess for union. The time to union varies depending on the location of the scaphoid fracture. The distal third fractures usually heal within 6-8 weeks, the middle third within 8-12 weeks, and the proximal third within 12-24 weeks. The increase in time to healing from distal to proximal is secondary to the tenuous blood supply and retrograde arterial flow.
Immobilisation of the wrist in a cast is a safe and reliable method for the treatment of acute fractures of the scaphoid since 90% to 95% will heal [7,8].
Surgical treatment
Indications for surgical treatment include:
- Fracture displacement greater than 1mm
- Intrascaphoid angle greater than 35 degrees (humpback deformity)
- Radiolunate angle of more than 15 degrees
- Transcaphoid perilunate dislocation
- Proximal pole fractures
- Comminuted fractures
- Non-displaced waist fractures in individuals who need to return quickly to work/sport.
- Nonunion or avascular necrosis
Surgical fixation of the fracture involves inserting a single or multiple screws. This can be done percutaneously or via an open procedure. Minimally displaced fractures can be treated by percutaneous screw fixation. Patients with non-unions and grossly displaced fractures need an open procedure.
Al-Ajmi et al [9] carried out a systematic review and meta-analysis of randomized controlled trials comparing surgical versus conservative treatments for acute undisplaced or minimally-displaced scaphoid fractures.
They found that surgical management of acute nondisplaced or minimally displaced fractures has not yet been proven to be superior to conservative management. Surgical treatment was found to be significantly better in terms of patient-reported functional outcome and grip strength, shorter time for bone union, and earlier return to work.
There was no statistically significant differences between the two treatments with regard to ROM and complications (malunion, nonunion, osteoarthritis, and symptomatic osteoarthritis), the need for further surgical treatment, avascular necrosis, infection, and procedure failure.
Shen et al [10] also carried out a meta-analysis of randomized controlled trials comparing operative and nonoperative treatment of acute undisplaced or minimally-displaced scaphoid fractures. This meta-analysis showed that operative treatment resulted in significantly better functional outcomes in the short term when compared with non-operative treatment. Futhermore, patients who accepted surgery had a more rapid return to work and surgery was advantageous in preventing delayed union of the fractures.
The meta-analysis, however, did not provide evidence supporting the routine use of operative treatment for all acute undisplaced or minimally displaced scaphoid fractures.
Complications
Several complications can result from treatment of scaphoid fractures.
1.Malunion
A step due to lateral displacement of a fracture fragment can result in a malunion. This is usually seen as a flexion or humpback deformity. Special investigations are needed to detect this malunion. Although the flexion deformity predominates, there may also be ulnar deviation and pronation of the distal fragment [11] and these are even more difficult to detect.
Cadaver studies show that a flexion deformity within the scaphoid causes loss of extension at the radiocarpal and midcarpal joints [12].
Amadio et al [13] using trispiral tomography, studied 46 wrists with healed scaphoid fractures. Of these 46 wrists, 20 had normal intrascaphoid angles of <35˚ and 83% of these had satisfactory clinical outcomes. Twenty-six wrists had abnormal intrascaphoid angles of >35˚, indicating a flexion deformity within the scaphoid. Of these only 27% had satisfactory clinical results as judged by function, pain, movement and strength.
Jiranek et al [14] compared 13 patients with malunion ( lateral intrascaphoid angle of >45˚) and 13 patients with acceptable union. Both followed Russe procedures for a nonunion. They found that there was no significant difference in symptoms or function but the measurements of movement and strength were worse in patients with malunion. According to the criteria of Amadio et al [13], the 13 patients with malunion would have had a poor prognosis but 12 of them returned to a high level of function despite the deformity [14].
There are few publications on the clinical outcome of corrective osteotomy of the scaphoid to treat the malunion.
Nakamura, Imaeda and Miura [15] in 1991 described seven such operations with a mean follow-up of 29 months and all the patients had satisfactory outcome. All the osteotomies had united within three months.
Pain was relieved in six patients and diminished in one and both movement and grip strength had improved.
Lynch and Linscheid [16] reviewed five corrective scaphoid osteotomies performed between 1.5 and 19 years earlier. All had united at a mean of 5.5 months after the surgery. Pain was relieved completely in three patients and diminished in two. There was a non-significant slight improvement in wrist movement. Grip strength was markedly improved. Four of the five patients developed mild radioscaphoid arthritis.
There is no consensus as to whether corrective osteotomy should be undertaken for malunited scaphoid fractures.
Amadio et al [13] found post-traumatic arthritis in 14 of 26 patients with malunion and in patients with acceptable union only four of 20 developed OA.
Lynch and Linscheid [16] showed that corrective osteotomy does not prevent the development of osteoarthritis. It may, however, slow the process.
Jiranek et al [14] were of the opinion that corrective osteotomy is not justified in asymptomatic patients.
2.Nonunion
Nonunion is the most likely complication arising from missed scaphoid fractures. The risk is higher in patients with very displaced fractures and in patients with associated carpal fractures. The nonunion rates for scaphoid fractures vary between 5% and 15% [17].
Nonunions usually produce pain in the wrist when the hand is used. However some patients may remain pain free for many years.
There are 4 different patterns of presentation in patients with scaphoid nonunions [13,18]:
1. Patients are treated and followed up adequately and they develop nonunion.
2. Patients are treated but followed up inadequately. Radiographs taken at only three months after fracture cannot differentiate reliably between a union and a nonunion. A follow-up for at least six months is required.
Some patients are discharged prematurely in the belief that the fracture has united and they later present with pain due to a nonunion. Other patients default from follow-up and they remove the cast themselves.
3. Patients who were never treated because they did not see a doctor after the injury. Patient may sustain a minor wrist injury at some later date and an x-ray is done and it shows a nonunion.
4. In some patients the nonunion is discovered accidentally when an x-ray is done for some other reason. This is rare.
Osteoarthritis is inevitable and pain probable in patients with a nonunion, but this may not occur until several decades after the injury.
In a complete pseudarthrosis the two halves of the scaphoid move separately, and the edge of one can scrape the articular surface on the radius.
Osteoarthritis initially affects the joint between the radius and the distal fragment of the scaphoid, which is the rationale for radial styloidectomy in the treatment of scaphoradial OA. The next joint to be affected is the midcarpal joint between the capitate and the proximal scaphoid. The joints between the radius and the proximal fragment of the scaphoid and between the radius and the lunate are rarely affected.
Nonunions of the scaphoid are treated by bone grafting. There are relatively few papers that have assessed the success of the procedure as judged by relief of pain. Pain relief is the prime purpose of the operation. There is often a striking discrepancy between the clinical and radiological outcomes [19]. Some patients have pain relief despite the persistence of the nonunion. This may be because a more stable fibrous union has been achieved following the surgery or because the operation has resulted in some restriction of movements of the wrist [14].
Most patients, in whom the operation fails, continue to have symptoms. Some patients in whom union occurs continue to have pain. This pain may be due to some other abnormality in the wrist. The pain might be due to a malunion.
Lindström and Nyström [20] were of the opinion that “the best indication for stabilising surgery is the totally asymptomatic patient in whom no sign of arthrosis can be found”. This is based on the assumption that success in achieving union will prevent osteoarthritis. The likelihood of subsequent osteoarthritis is somewhere between 5% and 100%. Most series report that failure to achieve union occurs in about 20% of patients.
The case for a prophylactic operation in patients with a nonunion to prevent osteoarthritis is not strong. It may result in reduced movement at the wrist. One in five will fail to achieve union and some of the remaining four will still develop osteoarthritis. A preventative operation is more appropriate in younger patients. The operation is more likely to be successful with nonunion at the waist than at the proximal pole.
3.Avascular necrosis
The incidence of avascular necrosis following a scaphoid fracture is approximately 30-40%. This is most likely to affect the proximal pole of the scaphoid.
Avascular necrosis (AVN) may be associated with long standing nonunion of proximal pole fractures, especially when associated with previous surgery.
AVN of scaphoid is usually difficult to diagnose radiographically and therefore it is usually necessary to assess vascularity of the proximal pole at the time of surgery. The absence of punctate bleeding in the proximal fragment after debridement is the best indicator of AVN. Following debridement, punctate bleeding should be present from the surface of the scaphoid while the tourniquet remains elevated.
Plain radiographs tend to underestimate the presence of AVN. The radiographic indicators of AVN include:
- Ground-glass appearance or increased bone density
- Loss of trabecular pattern;
- Cystic changes
- Subchondral collapse and fragmentation
The radiographic classification for AVN is as follows:
Stage 0: none
Stage 1: patchy areas of radiodensity of proximal pole
Stage 2: involvement of entire proximal pole
Stage 3: AVN with carpal collapse
An MRI is often used for diagnosis of AVN. Numerous early studies reported that unenhanced MRI was accurate for detecting AVN in the proximal pole of the scaphoid in patients with fracture nonunions [21].
One of those early studies suggested that, although T1-weighted images were sensitive for detecting AVN in the carpal bones, the findings were not specific. Hence, the authors advocated using decreased signal intensity on T2-weighted images which is more specific for the diagnosis.
Cerezal et al [22] in 2000 reported that the global accuracy of unenhanced MRI in categorizing the vascular status of the proximal scaphoid was only 68% and the global accuracy of gadolinium-enhanced imaging was 83%.
Nonunion with AVN of the scaphoid is treated with vascularised bone graft which is usually taken from the distal radius.
In a meta-analysis by Merrell et al [23], in which 36 studies were included, the union rate in the presence of proximal pole AVN was found to be 88% after vascular bone graft, while it was found to be 47% in patients treated with non vascularised bone graft.
Reference
- Hove LM. Epidemiology of scaphoid fractures in Bergen, Norway. Scand J Plast Reconstr Surg Hand Surg. 1999 Dec;33(4):423-6.
- Dias J et al. Scaphoid Waist Internal Fixation for Fractures Trial (SWIFFT) protocol: a pragmatic multi-centre randomised controlled trial of cast treatment versus surgical fixation for the treatment of bi-cortical, minimally displaced fractures of the scaphoid waist in adults. BMC Musculoskelet Disord. 2016 Jun 04;17:248.
- Mallee et al. Computed tomography versus magnetic resonance imaging versus bone scintigraphy for clinically suspected scaphoid fractures in patients with negative plain radiographs. Cochrane Database Syst Rev. 2015 Jun 05;(6):CD010023.
- Karantanas et al. The role of MR imaging in scaphoid disorders. Eur Radiol. 2007 Nov;17(11):2860-71.
- Yin ZG, Zhang JB, Kan SL, Wang XG. Diagnostic accuracy of imaging modalities for suspected scaphoid fractures: meta-analysis combined with latent class analysis. J Bone Joint Surg Br. 2012 Aug;94(8):1077-85.
- Dias JJ, Wildin CJ, Bhowal B, Thompson JR. Should acute scaphoid fractures be fixed? A randomized controlled trial. J Bone Joint Surg Am. 2005 Oct;87(10):2160-8.
- Duppe H, Johnell O, Lundborg G, Karlsson M, Redlund-Johnell I. Long-term results of fracture of the scaphoid: a follow-up study of more than thirty years. J Bone Joint Surg [Am] 1994;76-A:249-52.
- Kozin SH. Internal fixation of scaphoid fractures. Hand Clin 1997; l3:573-86.
- Al-Ajmi et al. A Systematic Review and Meta-analysis of Randomized Controlled Trials Comparing Surgical versus Conservative Treatments for Acute Undisplaced or Minimally-Displaced Scaphoid Fractures. Clinics in Orthopedic Surgery • Vol. 10, No. 1, 2018.
- Shen L, Tang J, Luo C, Xie X, An Z, Zhang C (2015) Comparison of Operative and Non-Operative Treatment of Acute Undisplaced or Minimally-Displaced Scaphoid Fractures: A Meta-Analysis of Randomized Controlled Trials. PLoS ONE 10(5): e0125247; 2015. https://doi.org/10.1371/journal.
- Fernandez DL, Martin CJ, Gonzalez del Pino J. Scaphoid mal-union: the significance of rotational malalignment. J Hand Surg [Br] 1998;23-B:771-5.
- Burgess RC. The effect of simulated scaphoid malunion on wrist motion. J Hand Surg [Am] 1987;12-A:774-6.
- Amadio PC, Berquist TH, Smith DK, et al. Scaphoid malunion. J Hand Surg [Am] 1989;14-A:679-87.
- Jiranek WA, Ruby LK, Millender LB, Bankoff MS, Newberg AH. Long-term results after Russe bone-grafting: the effect of malunion of the scaphoid. J Bone Joint Surg [Am] 1992;74-A:1217-28.
- Nakamura P, Imaeda T, Miura T. Scaphoid malunion. J Bone Joint Surg [Br] 1991; 73-B:134-7.
- Lynch NM, Linscheid RL. Corrective osteotomy for scaphoid malunion: technique and long-term follow-up evaluation. J Hand Surg [Am] 1997;22-A:35-43.
- Pao VS, Chang J. Scaphoid nonunion: diagnosis and treatment. Plast Reconstr Surg 2003;112:1666–1676.
- Prosser GH, Isbister ES. The presentation of scaphoid nonunion. Injury 2003;34: 65-7.
- Barton NJ. Experience with scaphoid grafting. J Hand Surg [Br] 1997;22-B:153-60.
- Lindström F, Nyström Å. Natural history of scaphoid nonunion, with special reference to “asymptomatic” cases. J Hand Surg [Br] 1992;17-B:697-700.
- Fox at el. Assessment of Scaphoid Viability With MRI: A Reassessment of Findings on Unenhanced MR Images. AJR:195, October 2010.
- Cerezal L, Abascal F, Canga A, García-Valtuille R, Bustamante M, del Piñal F. Usefulness of gadolinium-enhanced MR imaging in the evaluation of the vascularity of scaphoid nonunions. AJR 2000; 174:141–149.
- Merrell GA, Wolfe SW, Slade JF III. Treatment of scaphoid nonunions: quantitative meta-analysis of the literature. J Hand Surg Am 2002;27:685–691.
No comments:
Post a Comment