Modalities for Treatment of Pain
DR KS Dhillon
The International Association for the Study of Pain (IASP) has defined pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage” [1]. There are two broad categories of pain;
- Somatic Pain: This result from the activation of nociceptors that are sensitive to noxious stimuli in cutaneous or deep tissues. The pain experienced is described as constant, aching, and gnawing.
- Visceral Pain: This is also mediated by nociceptors. The pain is described as deep, aching, and colicky. It is poorly localized and often referred to cutaneous sites, which may be tender.
The five most common types of pain include:
- Acute pain
- Chronic pain
- Neuropathic pain
- Nociceptive pain
- Radicular pain
Acute pain
Acute pain is a sudden, sharp pain that lasts less than 3 months. Acute pain tends to be related to an injury or a temporary illness. It typically subsides after the injury heals or the illness subsides. Acute pain from an injury can evolve into chronic pain if the injury doesn’t heal properly or if the pain signals malfunction.
Chronic pain
Chronic pain is ongoing pain that lasts longer than 3 months. This pain is considered a disease state and affects 1 out of 5 adults. Chronic pain is difficult to diagnose and can be misdiagnosed. Chronic pain is caused by an underlying issue. Some of the conditions that produce chronic pain include headaches, arthritis, cancer, nerve pain, back pain, and fibromyalgia. Chronic pain is longer in duration and can be constant or intermittent.
Neuropathic pain
Neuropathic pain results from damage to nerves or other parts of the nervous system. The pain is shooting, stabbing, or burning in nature. Sometimes it feels like pins and needles. It can affect sensitivity to touch and it makes individuals have difficulty feeling hot or cold sensations. Neuropathic pain is a common type of chronic pain. It can be intermittent and it can also be so severe that it makes performing daily tasks difficult.
Nociceptive pain
Nociceptive pain is a type of pain caused by damage to body tissue that is caused by injury. People often describe it as being a sharp, achy, or throbbing pain. This type of pain is often experienced in the muscles, joints, skin, tendons, and bones. Such pain can be both acute and chronic.
Radicular pain
Radicular pain is a very specific type of pain that occurs when the spinal nerve gets compressed or inflamed. The pain radiates along the distribution of the nerve or nerve root. It can radiate from the back to the lower limbs or from the neck to the upper limbs. Individuals with radicular pain can experience tingling, numbness, and muscle weakness.
Pain scores
The unidimensional pain intensity scales commonly used are:
• Numeric Rating Scale (NRS),
• Visual Analog Scale (VAS),
• Verbal Rating / Descriptor Scale (VRS/VDS).
The VAS is the most widely used tool for estimating both severity of pain and to judge the extent of pain. The patient is asked to select a point on a line drawn between two ends to express how intense he/she perceives pain. The VAS is a continuous scale comprised of a horizontal or vertical line, usually 100 mm long, anchored by two verbal descriptors i.e., “no pain” and “worst imaginable pain”-Fig 1.
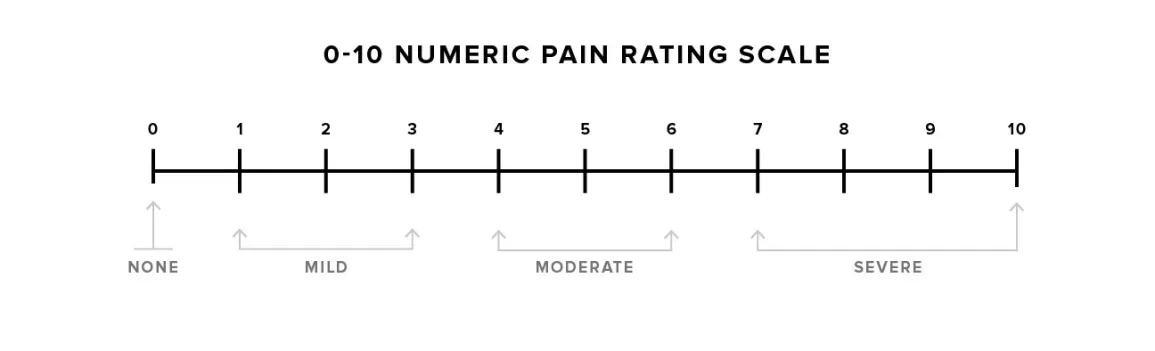
Figure 1
Pain management
Pain management should be carried out using a multimodal approach. It should consist of treatments from one or more clinical disciplines that are incorporated
into an overall treatment plan. This allows for different approaches to address the pain problem. Multidisciplinary approaches address different aspects of pain including psychosocial effects on the patient [2,3,4]. Such a coordinated, integrated approach reduces pain severity, improves mood and overall quality of life, and improves function [5,6].
Opioid and nonopioid analgesics are the main drugs used to treat pain. Antiseizure, antidepressants and other central nervous system (CNS)–active drugs are also used for chronic or neuropathic pain and can be first-line therapy for some conditions. Nerve stimulation, neuraxial infusion, and neural blockade can help in some patients.
Cognitive-behavioral interventions can reduce pain and pain-related disability and help patients cope with the pain. These interventions include counseling the patient to develop personal coping strategies and counseling the patients and their families to work together to manage pain.
Nonopioid Analgesics
Nonsteroidal anti-inflammatory drugs (NSAIDs) and acetaminophen are effective for mild to moderate pain. Most of the NSAIDs are given orally. Ibuprofen, ketorolac, diclofenac, and acetaminophen can be given parenterally. The advantage of using nonopioids is that they do not cause physical dependence or tolerance.
Acetaminophen has no antiplatelet effects and no anti-inflammatory effects and does not cause gastric irritation.
Aspirin is the cheapest NSAID, but unfortunately, it has irreversible antiplatelet effects and it increases the risk of gastrointestinal (GI) bleeding.
NSAIDs have analgesic and anti-inflammatory effects as well as antiplatelet effects. They inhibit cyclooxygenase (COX) enzymes and hence reduce the production of prostaglandins. There are several classes of NSAIDs, which have different mechanisms and adverse effects (Fig 1):
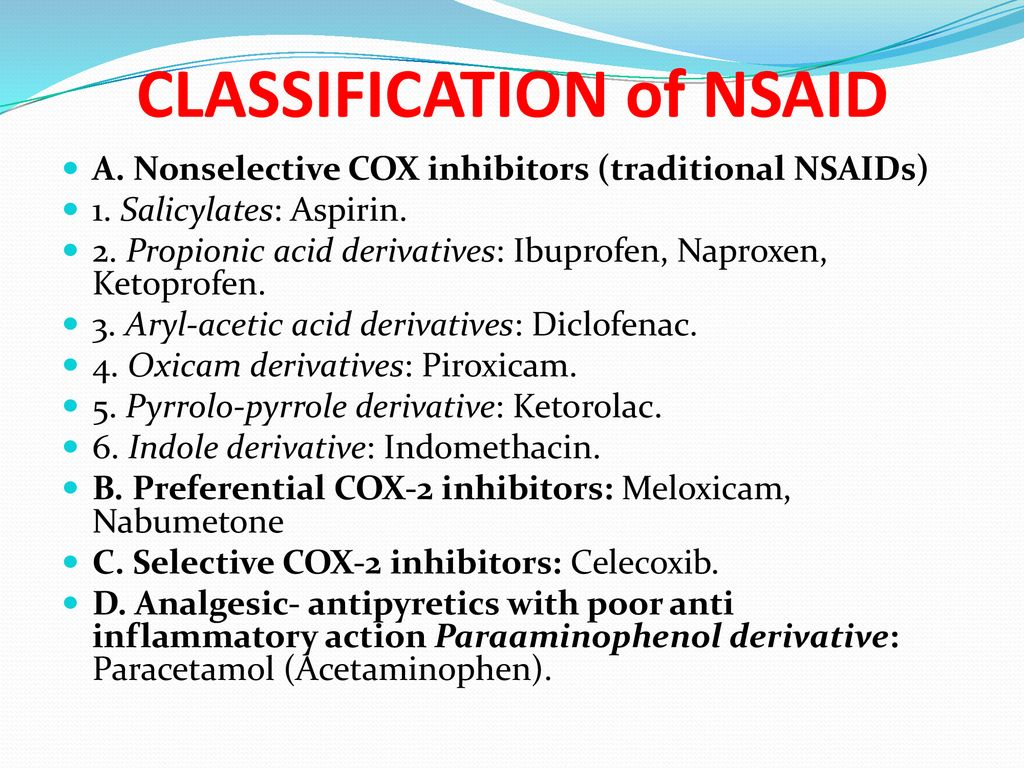
Fig 1.
There are 2 types of COX inhibitors i.e nonselective COX inhibitors (eg, ibuprofen, naproxen) and selective COX-2 inhibitors (coxibs; eg, celecoxib)
Both the COX inhibitors are effective analgesics. The coxibs have the lowest risk of gastric ulceration and gastritis.
COX-2 inhibition has a prothrombotic effect that can increase the risk of myocardial infarction, claudication, and stroke. This effect varies with the type of drug, as well as by the dose and duration of use. The risk is very low with some nonselective COX inhibitors such as ibuprofen, naproxen, and coxibs. All NSAIDs should be used cautiously in patients with clinically significant atherosclerosis or multiple cardiovascular risk factors because of the potential for prothrombotic effects of all NSAIDs. The use of NSAIDs can be associated with renal insufficiency, hypertension, and cardiac-related events.
There are no significant side effects if NSAIDs are used for a short duration. Whenever therapy is likely to be long-term (eg, months) some clinicians use a coxib first because the risk of GI adverse effects is lower. Coxib is used in patients who are predisposed to GI adverse effects, such as older patients, patients taking steroids, and those with a history of peptic ulcer disease or gastritis.
All NSAIDs should be used cautiously in patients with renal insufficiency.
If a lower dose provides inadequate analgesia, a higher dose is given, up to the conventional safe maximum dose. If with higher dose analgesia remains inadequate, the drug should be stopped. During long-term NSAID therapy, it is prudent to monitor for occult blood in stool and changes in the blood count, electrolytes, and hepatic and renal function.
Acetaminophen can be effective for the treatment of mild to moderate pain. The use of acetaminophen can be associated with dose-dependent liver toxicity, especially if the drug is taken at high doses, with alcohol, or by those with liver disease [7].
Opioid Analgesics
Opioid is a term used for natural or synthetic substances that bind to specific opioid receptors in the central nervous system (CNS). Opioids are also called narcotics. Opioids have both sleep-inducing and analgesic effects.
Some opioids have both agonist and antagonist actions. The potential for abuse among individuals with a known history of abuse or addiction is lower with agonist-antagonists such as buprenorphine and butorphanol than with pure agonists such as morphine, oxycodone, and hydromorphone. Agonist-antagonist drugs have a ceiling effect for analgesia and they induce a withdrawal syndrome in individuals already physically dependent on opioids.
Opioid analgesics have proven efficacy in the treatment of pain. The risk of opioid misuse has to be kept in mind when using opioids for the treatment of pain. Underuse of opioids can result in needless pain and suffering.
Some of the reasons for underusage leading to undertreatment include:
- Underestimation of the effective dose
- Overestimation of the risk of adverse effects
Simultaneous treatment of the condition causing the pain can limit the duration of severe pain and the need for opioids.
For acute pain, short-acting (immediate-release) pure agonist drugs are used at the lowest effective dosage and for a short time. The Centers for Disease Control and Prevention (CDC) guidelines recommend 3 to 7 days[8]. Using opioids at higher doses and for a longer time increases the risk of needing long-term opioid therapy, adverse effects, and misuse of opioids. Opioids should not be withheld when treating cancer pain. In such cases, adverse effects can be prevented or managed, and addiction is not much of a concern.
There is no good evidence to support the use of opioids for the long-term treatment of chronic pain due to non-terminal disorders. Long-term opioid therapy can result in adverse effects such as addiction, overdose, respiratory depression, and death. In patients with chronic pain due to non-terminal disorders, lower-risk nonopioid therapies should be tried before opioids.
If nonopioid therapy has been unsuccessful in patients with chronic pain due to non-terminal disorders, opioid therapy can be considered. In such cases, opioids are used in combination with nonopioid therapies. The goals, expectations, and risks of treatment should be explained to the patient. The patient should also be counseled about the misuse of the drug.
When treatment with opioids is appropriate the chronic pain can be treated with long-acting formulations. Long-acting formulations should be avoided in opioid-naive patients because of a higher risk of serious adverse effects.
Patients on long-term (more than 3 months) opioid therapy are regularly assessed for pain control, functional improvement, adverse effects, and signs of misuse of the drug.
Opioid therapy should be tapered and stopped if the following occur:
- Patients continue to have persistent severe pain despite increasing opioid doses.
- Patients do not adhere to the treatment protocol
- Physical or mental function does not improve.
All patients treated with opioids for more than a few days develop physical dependence i.e they develop withdrawal symptoms when a drug is stopped. They also develop tolerance i.e they develop decreased response to the same dose of a drug that is used repeatedly. Therefore, opioids should be used for as short periods as possible. In patients who have developed dependence, the dose should gradually be tapered to control withdrawal symptoms when opioids are no longer needed.
Different opioids have different potencies based on their ability to bind to opioid receptors. Knowing the interrelationship of these potencies is essential if patients need to be transitioned from one opioid to another or from an oral to an IV form. A 30 mg of oral morphine is equivalent to:
- 10 mg of IV morphine (a 3:1 oral-to-IV ratio)
- 7.5 mg of oral hydromorphone
- 20 mg of oral oxycodone
Route of administration
In patients who are able to tolerate oral medications, oral opioids may be used for the treatment of acute pain. Especially in patients who need medications for a long time, the oral or transdermal route is preferred. Both these routes provide stable blood levels.
Sublingual formulations of fentanyl are available. Lozenges can be used for sedation in children.
The intravenous (IV) route provides the most rapid onset but the duration of analgesia is short. Sometimes continuous IV infusion, with patient-controlled supplemental doses are used. This approach is used most often for postoperative pain control.
The intramuscular (IM) route provides analgesia for a longer duration than IV but the IM injections can be painful, and absorption can be erratic.
Intraspinal opioids can provide relief, which is prolonged when a hydrophilic drug such as morphine is used. They are typically used perioperatively.
Dosing
In opioid-naive patients, the initial dose is usually the lowest available starting dosage of the immediate-release formulation. It is increased incrementally by the smallest amount practical until analgesia is satisfactory or adverse effects set in. Long-acting opioids are not used as first-line treatment in opioid-naive patients. Nonopioid analgesics are usually given concomitantly.
Opioid-naive older patients typically require lower doses than younger patients because older patients are more sensitive to opioids and are predisposed to side effects.
When opioids are given parentally the patient must be monitored for sedation and respiratory depression. Short-acting opioids are used initially. The doses of opioids for patients with chronic noncancer pain are typically decided case by case.
Patients in hospitals with severe pain and whose oral analgesics are inadequate can be given patient-controlled IV analgesia. The physician decides on the amount and interval of the bolus dose to be administered. A bolus dose of 1 mg morphine or 0.2 mg hydromorphone as often as every 6 minutes is provided when the patient presses a button. Only the patient is allowed to press the administration button.
A baseline infusion of morphine, 0.5 to 1 mg/hour can be used. A baseline infusion should be used with caution, and it should only be used in patients who are alert enough to manage patient-controlled analgesia. Patients with prior opioid exposure or those with chronic pain require a higher bolus and baseline infusion dose.
Patients who have dementia cannot use patient-controlled analgesia, nor can young children.
Treatment of chronic pain with opioids is only done when other options have been tried and found to be not effective. The effective opioid dose can remain constant for prolonged periods when used for long-term treatment of chronic pain. There will be some patients who need intermittent dose escalation when the pain gets more severe as in patients with progressive neoplasm.
Methadone has the highest rate of opioid-induced deaths. It should only be prescribed by practitioners trained in its use. It should be started at a low dose and its use should be closely monitored. Methadone can prolong the cardiac QT interval hence the QTc interval should be assessed by ECG before methadone initiation.
Adverse effects
The common adverse effects at the start of therapy with opioids include:
- Sedation and mental clouding
- Respiratory depression
- Constipation
- Nausea and vomiting
- Itch
- Myoclonus
Opioids tend to have more adverse effects such as constipation and sedation in older patients. The risk of falls is high in such patients. Opioids can cause urinary retention in men with prostatic hyperplasia.
In patients with the following disorders, opioids should be used cautiously:
- COPD because of the risk of respiratory depression
- Hepatic disorders because drug metabolism is delayed
- Untreated obstructive sleep apnea because of risk of respiratory depression
- Some neurologic disorders, such as dementia and encephalopathy, because of risk of delirium
- Severe renal insufficiency because metabolites can accumulate and cause problems
Sedation is a common side effect of opioids. Patients should avoid driving and make sure they do not fall. In patients in whom sedation impairs the quality of life, certain stimulant drugs may be given intermittently or regularly to some patients.
Methylphenidate at a dose of 5 to 10 mg orally once or twice a day, titrated by 5 mg every 3 days to a maximum dose of 40 mg a day can be given to such patients.
Dextroamphetamine at an initial dose of 2.5 mg orally once or twice a day can alternatively be used. Modafinil at an initial dose of 100 mg orally for 3 to 7 days, then 200 mg orally once a day is another alternative for these patients.
In some patients, caffeine-containing beverages provide enough stimulation. Stimulants can also potentiate analgesia.
The risk of overdose or respiratory depression is higher when patients are taking other sedatives, such as muscle relaxants, benzodiazepines, gabapentin, and alcohol. The risk is highest with benzodiazepines. Benzodiazepines should not be used with opioid therapy. The risk is also high when patients have comorbidities that affect hepatic or renal metabolism.
Risk factors for respiratory depression also include:
- History of renal disease, heart failure, stroke, or chronic pulmonary disease
- Untreated or undertreated chronic obstructive pulmonary disease or obstructive sleep apnea
- Psychiatric disorders
- Substance use disorder
- Concurrent use of psychoactive drugs
- Use of long-acting opioids, high-dose opioids, or methadone
Hence, to reduce the risk for respiratory depression sleep apnea should be treated, patients should be advised not to drink alcohol, benzodiazepines should not be prescribed and long-acting opioids should be avoided.
Nausea can be treated with the following medications:
- Hydroxyzine 25 to 50 mg orally every 6 hours
- Ondansetron 4 mg orally or IV every 8 hours
- Metoclopramide 10 to 20 mg orally every 6 hours
- Prochlorperazine 10 mg orally or 25 mg rectally every 6 hours
Itching is caused by histamine release and can be treated with antihistamines. Diphenhydramine 25 to 50 mg orally or IV can be given to the patient. In hospitalized patients, nalbuphine 2.5 to 5 mg IV every 4 hours is more effective than diphenhydramine.
Constipation is common in patients who take opioids for more than a few days. It is more common in the elderly and immobile patients. Preventive treatment should be started with more fluids and more fiber intake. Laxatives such as senna and polyethylene glycol can be given daily. A drug that is specific for opioid-induced constipation can also be used.
Effective drugs include:
- Naloxegol 25 mg orally once a day
- Methylnaltrexone 12 mg/0.6mL subcutaneously or 450 mg orally once a day
- Lubiprostone 24 mcg orally 2 times a day
Persistent constipation can be treated with oral magnesium citrate 240 ml daily, or oral lactulose 15 ml twice daily. Some patients will require regular enemas.
For urinary retention, double voiding or using the Credé method during voiding can help. Some patients benefit from an alpha-adrenergic blocker such as oral tamsulosin 0.4 mg daily.
Neuroendocrine effects are also possible. Typically reversible hypogonadism can be seen. Symptoms can include loss of libido, fatigue, infertility due to low levels of sex hormones, and, in women, amenorrhea. Low levels of androgens also lead to osteoporosis and hence patients taking long-term opioid therapy would require intermittent bone density testing.
Opioid misuse and abuse
Opioids are the leading cause of fatal drug overdose and accidental death in the US. The risk of fatal drug overdose increases significantly when opioids are used with benzodiazepines.
The misuse of opioids may be intentional or unintentional. Abuse refers to recreational or nontherapeutic use of opioids for euphoria and other psychotropic effects. About one-third of the patients taking long-term opioids for chronic pain may misuse the prescribed opioids.
Addiction refers to compulsive use despite harm and negative consequences and it is typically marked by impaired control and craving. Discontinuation of the drug or a significant decrease in the dose can cause withdrawal symptoms.
Rather than addiction, opioid use disorder is the preferred term. Opioid use disorder refers to a compulsive, long-term self-administration of opioids for nontherapeutic purposes that leads to significant distress or impairment.
Opioid use disorder is diagnosed if 2 or more of the following are observed over a period of 12 months:
- Taking opioids in larger amounts or for a longer time than is needed
- Persistently desiring or unsuccessfully attempting to control or decrease opioid use
- Spending a great deal of time trying to obtain or use opioids, or recover from opioid effects
- Having a craving or strong desire to use opioids
- Using opioids repeatedly resulting in failing to meet daily obligations at home, work, or school
- Continuing to use opioids despite having persistent or recurrent social or interpersonal problems due to the opioid use
- Giving up or reducing important work, social, or recreational activities because of opioid use
- Having tolerance to opioids
- Having opioid withdrawal symptoms
- Continuing to use opioids in physically hazardous situations
- Continuing to use opioids despite having a persistent or recurrent physical or psychologic disorder caused or worsened by opioids
Tolerance and withdrawal symptoms also occur in patients who take opioids under medical supervision. Such tolerance and withdrawal symptoms are not considered as opioid use disorders.
There are several risk factors for developing opioid use disorder and these include:
- History of alcohol or drug abuse by the patient
- History of alcohol or drug abuse in the family
- Use of psychoactive drugs
- Current or past major psychiatric disorder
- Younger age, usually less than 45 years
All patients who are treated with opioids should be monitored closely to make sure that the opioid therapy is used safely. Monitoring should include periodic unannounced urine drug tests to check for the presence of the prescribed drug and the absence of illicit drugs.
Current recommendations for urine drug screening include:
- When a prescription is first given
- At least once a year
- More frequently if the risk is high or there is concern
Even when there are risk factors for developing an opioid use disorder, treatment can be continued. However, the clinicians should use more stringent measures to prevent abuse and addiction [9].
Some of these measures include:
- Only small amounts are prescribed each visit and frequent visits are required for refills
- Urine drug screening is carried out to monitor that the patient is adhering to treatment and to make sure that the patient is not diverting the drugs
- So-called “lost” prescriptions are not refilled
- Use of tamper-resistant opioid formulations to deter abuse by chewing or by crushing and injecting oral preparations
- Buprenorphine formulations are useful for analgesia since they have a ceiling effect on the risk of sedation and respiratory depression
Problematic patients are usually referred to a pain specialist or a substance use specialist.
When an opioid is first prescribed to a patient, the clinician should provide relevant information to the patient. If the patient develops opioid use disorder, the physician is responsible for offering and arranging evidence-based treatment.
All patients have to be told about the risks of combining opioids with alcohol and anxiolytics.
Opioid antagonists
Opioid antagonist is an opioid-like substance that binds to opioid receptors but produces little or no agonist activity. Opioid antagonists are used mainly to reverse symptoms of opioid overdose, especially respiratory depression. Some of these antagonists include:
1. Naloxone
Naloxone acts in less than 1 minute when given intravenously and slightly less rapidly when given IM. It can also be administered sublingually or endotracheally. Its duration of action is about 60 to 120 minutes. Opioid-induced respiratory depression usually lasts longer than the duration of antagonism; hence, repeated doses of naloxone and close monitoring are necessary.
The dose of naloxone for acute opioid overdosage is 0.4 mg IV every 2 to 3 minutes as needed and is titrated to adequate respiration. If repeated doses are required, the dose can be increased to a maximum of 2 mg IV per dose.
In patients receiving long-term opioid therapy, naloxone should be used only to reverse respiratory depression and must be given cautiously to avoid producing withdrawal symptoms or recurrent pain.
Naloxone is also available as an auto-injector (IM) and a nasal spray. A single spray of 2 or 4 mg in 0.1 mL is sprayed into one nostril. For the auto-injector, the dose is 2 mg injected IM or subcutaneously into the thigh.
2. Nalmefene is similar to naloxone. Its duration of action is about 4 to 8 hours. Nalmefene is sometimes used to ensure prolonged opioid reversal.
3. Naltrexone is an oral opioid antagonist. It is given as adjunctive therapy in opioid and alcohol addiction. It is long-acting and is generally well-tolerated.
Adjuvant Analgesic Drugs
There are other drugs that are used as analgesics. These include antiseizure drugs such as gabapentin, pregabalin, antidepressants like tricyclics, duloxetine, venlafaxine, bupropion, and many others. These drugs are most notably used for neuropathic pain.
Gabapentin is widely used for headache syndromes and neuropathic pain. Pregabalin is very similar to gabapentin but it has more stable pharmacokinetics. Dosing 2 times a day is as efficacious as dosing 3 times a day and it results in better compliance. Pregabalin is effective for neuropathic pain and fibromyalgia. There is some evidence that suggests it is effective as an anxiolytic as well.
The primary mechanism of action of tricyclic antidepressants, such as amitriptyline, nortriptyline, and desipramine, is blocking the reuptake of serotonin and norepinephrine. These drugs are effective for neuropathic pain, visceral pain syndromes, myofascial pain syndromes, some central neuropathic pain syndromes, and headache syndromes.
Duloxetine is also a serotonin and norepinephrine reuptake inhibitor. It is effective for diabetic neuropathic pain, chronic musculoskeletal pain (including low back pain), fibromyalgia, and chemotherapy-induced neuropathy. The effects and mechanism of action of Venlafaxine are similar to those of duloxetine.
Topical drugs such as capsaicin cream, topical NSAIDs, other compounded creams, and lidocaine 5% patch have little risk of adverse effects and are also used for pain.
Neural Blockade
Short-term and sometimes long-term pain relief can be obtained by interrupting nerve transmission in peripheral or central pain pathways with drugs or via physical methods.
Neuroablation or pathway ablation is rarely used. It is usually reserved for patients who have an advanced disorder and a short life expectancy.
Local anesthetic drugs for pain relief such as lidocaine can be given IV, subcutaneously, intrathecally, intrapleurally, transdermally, or even epidurally. Epidural analgesia using local anesthetics or opioids is often used for postoperative pain. In patients with localized pain and a short life expectancy, long-term epidural drug administration is occasionally used. An implanted pump is often used for long-term neuraxial infusion, via the intrathecal route.
In neuroablation, the nociceptive pathways are interrupted surgically or by using radiofrequency or microwave energy, cryoablation, or caustic substances such as phenol or high-concentration alcohol. Neuroablation is usually more effective for somatic pain than for visceral pain.
Neuroablation procedures are commonly used to treat axial spinal pain. These procedures involve radiofrequency ablation of the medial branches of the dorsal spinal root rami that innervate the facet joints or ablation of the lateral branches that innervate the sacroiliac joint. Neroablation of the genicular nerve is also carried out for refractory knee pain. Neroablation of the articular sensory branches of the obturator and femoral nerves has also been carried out for hip pain. For shoulder pain, neuroablation of the articular sensory branches of the suprascapular, axillary, and lateral pectoral nerves can be carried out.
Neuromodulation
Stimulation of neural tissues can reduce pain by activating endogenous pain pathways. Certain types of neuropathic pain such as that after failed back surgery, and in patients with complex regional pain syndrome can be treated using an electrode placed epidurally to stimulate the spinal cord.
Transcutaneous electrical nerve stimulation (TENS) is also used to treat pain. It uses a low current at a low frequency to help treat pain. Studies of its efficacy are, however, lacking in number and design, with high risks of bias commonly reported [10]. An evaluation of 49 systematic reviews, randomized controlled trials (RCTs), and observational studies found that there is insufficient evidence to assess the effectiveness of TENS for acute low-back pain [11].
There are individual studies that have investigated the effectiveness of TENS for postpartum pain, phantom limb pain, and knee osteoarthritis [12].
Despite the fact that there is limited evidence of efficacy, partially stemming from a lack of large RCTs, TENS is considered a safe self-care option for patients with appropriate education.
Some of the advances in neuromodulation techniques and technologies include:
- High-frequency stimulation
- Burst spinal cord stimulation waveforms
- Dorsal root ganglion stimulation
- Small flexible peripheral nerve stimulators
- Improved MRI compatibility, which has greatly expanded the clinical situations in which neuromodulation can be used
High-frequency stimulation is effective in patients with neuropathic limb pain.
A more focused neuromodulation treatment is dorsal root ganglion stimulation. It treats localized neuropathic pain within limited dermatomes.
Peripheral nerve stimulation is frequently used to treat intractable neuropathic pain when a single peripheral nerve is involved. Some examples include post herniorrhaphy pain syndrome, headache syndromes such as occipital neuralgia, and meralgia paresthetica. It is also used to stimulate branches of the axillary nerve to treat hemiplegic shoulder pain after a stroke. Peripheral nerve stimulation can be useful in treating postoperative pain during the first several weeks after total knee replacement, anterior cruciate ligament surgery, and foot surgery.
Peripheral nerve stimulation involves the percutaneous insertion of a small, thin, flexible electrode leads next to the affected nerve. The leads are then connected to a stimulator, which is fixed to the skin adjacent to the leads.
Massage therapy
Massage therapy can be effective in reducing pain. There are several types of massage therapy, including shiatsu, Swedish, and deep tissue (myofascial release).
In Swedish massage, the therapist uses long strokes, deep circular movements, and kneading. Shiatsu massagers use their fingers, thumbs, and palm to apply pressure. Deep tissue massagers focus on myofascial trigger points, with attention on the deeper layers of tissues.
Traction
Traction is also a technique used to treat spinal pain. A review of the evidence, however, has failed to demonstrate the clinical effectiveness of traction as an effective, evidence-based best practice. The field in general lacks high-quality RCTs that examine the effectiveness of traction as an isolated treatment modality for low-back [13] or neck pain [14].
Cold and Heat
Cold and heat have been used in the treatment of a variety of acute and chronic pain conditions. The use of cold compress has long been a component of the RICE i.e rest, ice, compression, elevation, paradigm for the treatment of acute pain.
The effects and duration of this therapy are mitigated by the initial cause of the pain. Cold therapy, for instance, has been shown to decrease the pain of hip arthroplasty on the second day but not the first or third day after surgery and did not decrease blood loss from the surgery [15].
There is significant evidence for the efficacy and safety of heat wraps in specific conditions, most notably for acute low back pain. A review of nonpharmacologic therapies found that superficial heat had good evidence of efficacy for the treatment of acute low-back pain [16]. There is another review that found moderate evidence for heat wraps for both symptom and functional improvements [17].
Therapeutic ultrasound (TU)
Therapeutic ultrasound is believed to deliver heat to deep tissues for improved injury healing. A 2001 review by Robertson and Baker concluded that there was little evidence that TU is more effective than placebo for pain treatment in a range of musculoskeletal conditions [18].
More recent reviews of specific pain syndromes that are available from the Cochrane Database of Systematic Reviews reveal similar findings [19,20].
Bracing
Bracing has been discouraged in pain management because of fears of deconditioning and muscle atrophy. There is, however, some evidence that bracing (non-rigid brace) for at least short periods of time, may improve function and does not result in muscle dysfunction [21].
Behavioral Health Approaches
In recent decades, Pain management experts, in recent decades have recognized the important relationship between psychological health and pain [22,23,24]. Psychological factors play an important role in an individual’s experience and response to pain [25]. Psychological factors can affect treatment adherence, pain chronicity, and disability status [26].
Undiagnosed and untreated psychological concerns in individuals with pain are associated with decreased treatment adherence and increased disability [27].
Patients with chronic pain are also at increased risk for psychological distress.
Psychological interventions can play an important role in reducing disability in these patients. Behavioral health approaches should be considered a key component of multidisciplinary pain management.
Behavioral therapy (BT)
Behavioral therapy for pain focuses largely on identifying and reducing maladaptive pain behaviors and increasing adaptive behaviors. This is achieved by minimizing reinforcement of maladaptive behaviors and providing reinforcement of well behaviors. Avoidance behaviors are reduced through gradual exposure to fear-provoking stimuli such as exercises.
The main aim of BT in the treatment of pain is to improve function. Treatment with BT has been effective in reducing pain behaviors and distress and improving overall function. It can be more cost-effective than active physical treatment [28].
Cognitive behavioral therapy (CBT)
The aim of cognitive behavioral therapy is to reduce maladaptive behavior and improve overall function. Besides focusing on altering behavioral responses to pain, CBT also focuses on shifting cognitions and improving pain-coping skills [29].
Psychoeducation about the relationship between psychological factors such as thoughts, and feelings, and pain is carried out. Restructuring of maladaptive thought patterns and training in a variety of pain coping strategies is done. CBT can help improve self-efficacy, pain catastrophizing, and overall functioning [30,31].
CBT has been found to produce long-term improvements in patients with low-back pain and fibromyalgia [32].
Acceptance and commitment therapy (ACT)
Acceptance and commitment therapy is a form of CBT that teaches individuals to observe and accept thoughts and feelings, live in the present moment, and behave in a manner that serves an individual’s chosen values. ACT focuses on creating psychological flexibility through acceptance of psychological and physical experiences rather than by challenging them [33,34].
Mindfulness-based stress reduction (MBSR)
Mindfulness-based stress reduction is a mind-body treatment that is usually delivered in a group and it focuses on improving patients’ awareness and acceptance of their physical and psychological experiences through intensive training in mindfulness meditation [35].
Mindfulness meditation teaches individuals to self-regulate their pain and pain-related comorbidities by developing awareness and acceptance of present moment sensations, thoughts, and emotions [36,37].
MBSR is an effective intervention for helping individuals cope with a variety of pain conditions such as including low back pain, rheumatoid arthritis, and multiple sclerosis [38,39].
MBSR also has a definitely good impact on pain intensity sleep quality, fatigue, and overall physical functioning and well-being [40,41,42].
Emotional awareness and expression therapy (EAET)
Emotional awareness and expression therapy is an emotion-focused therapy for patients who suffer from centralized pain conditions following trauma. Here the patients are taught that their pain is exacerbated or maintained by unresolved emotional experiences that influence neural pathways involved in pain. The patients are taught to become aware of these unresolved experiences, that include suppressed or avoided trauma, conflict, and adversity. They are advised to express their emotions related to these experiences. Patients are able to learn that control over pain can be achieved through emotional awareness and expression.
Patients are encouraged to approach an experience rather than inhibit or avoid important emotions and interpersonal interactions. Research shows that EAET has a positive impact on pain intensity, pain interference, and depressive symptoms [43].
Self-regulatory or psychophysiological approaches
Self-regulatory or psychophysiological approaches include treatments such as hypnotherapy, biofeedback, and relaxation training. The mind-body connection is used to help patients with pain develop control over their physiologic and psychological responses to pain [23]. Biofeedback involves monitoring and providing real-time feedback about physiologic functions associated with the pain experience, such as heart rate, muscle tension, and skin conductance. The overall goal of biofeedback is to improve awareness and voluntary control over bodily reactions that are associated with pain exacerbations [44].
Biofeedback training has been effective for chronic headaches and migraine in children and adults [45]. Hypnotherapy and relaxation training involve altering attentional processes and heightening the experience of physical and psychological relaxation.
Relaxation training is often used in conjunction with biofeedback to enhance relaxation skills and increase physiological awareness [23]. Hypnotherapy is also used to manage cancer pain, arthritis, low-back pain, fibromyalgia, pain from SCD, temporomandibular joint pain, and other pain conditions [46]. As with relaxation training, hypnotherapy induces an altered state of consciousness guided by a hypnotherapist that focuses the individual’s attention to alter her or his experience of pain.
Access to Psychological Interventions
Many patients with pain receive inadequate care despite widespread understanding of the importance of psychological interventions in the management of pain [47,48].
There are several factors that contribute to this problem. These include
- Clinical barriers such as treatment accessibility, knowledge gaps, provider attitudes
- Health care system-related barriers such as cost and reimbursement issues
- Patient-related barriers such as stigma, and attitudinal variables
When access to providers and costs are limiting factors, low-cost and scalable approaches delivered through telehealth and internet technologies can provide a low-burden, effective alternative to traditional treatment approaches [49].
Brief telehealth and digitally delivered treatments allow broad patient access and yield outcomes that are similar to traditional in-person psychological interventions for chronic pain [50].
The patients and providers need to know about psychological treatments. Health professionals must have a sufficient understanding of the biopsychosocial model of Pain. They have to know how to appropriately assess and refer patients for behavioral treatment [51,52]. This can be achieved by improving training and education in pain management [53,54] and enhancing public awareness of the biopsychosocial aspects of pain [55].
References
- Raja SN, Carr DB, Cohen M, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976-1982. doi:10.1097/j.pain.0000000000001939
- Gatchel RJ, McGeary DD, McGeary CA, Lippe B. Interdisciplinary chronic pain management: past, present, and future. Am Psychol. 2014;69(2): 119-130. doi:10.1037/a0035514
- Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133(4):581-624. doi:10.1037/0033- 2909.133.4.581.
- Staats PS, Hekmat H, Staats AW. The psychological behaviorism theory of pain: A basis for unity. Pain Forum. 1996;5(3):194-207. doi:10.1016/S1082- 3174(96)80031-6.
- Gatchel RJ, Okifuji A. Evidence-based scientific data documenting the treatment and cost-effectiveness of comprehensive pain programs for chronic nonmalignant pain. J Pain Off J Am Pain Soc. 2006;7(11):779-793. doi:10.1016/j.jpain.2006.08.005
- Oslund S, Robinson RC, Clark TC, et al. Long-term effectiveness of a comprehensive pain management program: strengthening the case for interdisciplinary care. Proc Bayl Univ Med Cent. 2009;22(3):211-214.
- Major JM, Zhou EH, Wong H-L, et al. Trends in rates of acetaminophen-related adverse events in the United States. Pharmacoepidemiol Drug Saf. 2016;25(5):590-598. doi:10.1002/pds.3906
- Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic Pain--United States, 2016. JAMA. 2016;315(15):1624-1645. doi:10.1001/jama.2016.1464.
- Babu KM, Brent J, Juurlink DN: Prevention of opioid overdose. N Eng J Med 380:2246–2255, 2019. doi: 10.1056/NEJMra1807054.
- Vance CG, Rakel BA, Dailey DL, Sluka KA. Skin impedance is not a factor in transcutaneous electrical nerve stimulation effectiveness. J Pain Res. 2015;8:571-580.
- McIntosh G, Hall H. Low back pain (acute). BMJ Clin Evid. 2011;2011. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3217769/.
- Pain Management Best Practices Inter-Agency Task Force Report (DRAFT FINAL REPORT 5/6/2019) at https://www.hhs.gov/sites/default/files/pain-mgmt-best-practices-draft-final-report-05062019.pdf.
- Clarke J, van Tulder M, Blomberg S, de Vet H, van der Heijden G, Bronfort G. Traction for low back pain with or without sciatica: an updated systematic review within the framework of the Cochrane collaboration. Spine. 2006;31(14):1591-1599.
- Graham N, Gross A, Goldsmith CH, et al. Mechanical traction for neck pain with or without radiculopathy. Cochrane Database Syst Rev. 2008; (3): CD006408.
- Ni S-H, Jiang W-T, Guo L, et al. Cryotherapy on postoperative rehabilitation of joint arthroplasty. Knee Surg Sports Traumatol Arthrosc Off J ESSKA. 2015;23(11):3354-3361. doi:10.1007/s00167-014-3135-x.
- Chou R, Huffman LH, American Pain Society, American College of Physicians. Nonpharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline. Ann Intern Med. 2007;147(7):492-504.
- McIntosh G, Hall H. Low back pain (acute). BMJ Clin Evid. 2011;2011. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3217769/.
- Robertson VJ, Baker KG. A review of therapeutic ultrasound: effectiveness studies. Phys Ther. 2001;81(7):1339-1350.
- Ebadi S, Henschke N, Nakhostin Ansari N, Fallah E, van Tulder MW. Therapeutic ultrasound for chronic low-back pain. Cochrane Database Syst Rev. 2014;(3):CD009169.
- Rutjes AW, Nüesch E, Sterchi R, Jüni P. Therapeutic ultrasound for osteoarthritis of the knee or hip. Cochrane Database Syst Rev. 2010;(1):CD003132.
- Azadinia F, Ebrahimi E Takamjani, Kamyab M, Parnianpour M, Cholewicki J, Maroufi N. Can lumbosacral orthoses cause trunk muscle weakness? A systematic review of literature. Spine J. 2017 Apr;17(4):589-602. doi: 10.1016/j.spinee.2016.12.005. Epub 2016 Dec 14. PMID: 27988341.
- Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133(4):581-624.
- Kerns RD, Sellinger J, Goodin BR. Psychological treatment of chronic pain. Annu Rev Clin Psychol. 2011;7:411-434. doi:10.1146/annurev-clinpsy 090310-120430
- Manchikanti L, Fellows B, Singh V. Understanding psychological aspects of chronic pain in interventional pain management. Pain Physician. 2002;5(1):57-82.
- Chou R, Qaseem A, Snow V, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of physicians and the American Pain Society. Ann Intern Med. 2007;147(7): 478-491.
- Kligler B, Bair MJ, Banerjea R, et al. Clinical Policy Recommendations from the VHA State-of-the-Art Conference on Non-Pharmacological Approaches to Chronic Musculoskeletal Pain. J Gen Intern Med. 2018; 33(Suppl 1):16-23. doi:10.1007/s11606-018-4323-z.
- Kellezi B, Coupland C, Morriss R, et al. The impact of psychological factors on recovery from injury: a multicentre cohort study. Soc Psychiatry Psychiatr Epidemiol. 2017;52(7):855-866. doi:10.1007/s00127-016-1299-z.
- McCracken LM, Turk DC. Behavioral and cognitivebehavioral treatment for chronic pain: outcome, predictors of outcome, and treatment process. Spine. 2002;27(22):2564-2573.
- Kaiser RS, Mooreville M, Kannan K. Psychological Interventions for the Management of Chronic Pain: a Review of Current Evidence. Curr Pain Headache Rep. 2015;19(9):43.
- Jensen MP, Turner JA, Romano JM. Changes in beliefs, catastrophizing, and coping are associated with improvement in multidisciplinary pain treatment. J Consult Clin Psychol. 2001;69(4):655-662.
- Turner J, Jensen M, Romano J. Do beliefs, coping, and catastrophizing independently predict functioning in patients with chronic pain? Pain. 2000;85(1-2):115-125.
- Skelly AC, Chou R, Dettori JR, et al. Noninvasive Nonpharmacological Treatment for Chronic Pain: A Systematic Review. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018. http://www.ncbi.nlm.nih.gov/books/NBK519953/.
- McCracken LM, Vowles K. Acceptance and Commitment Therapy and Mindfulness for Chronic Pain: Model, Process, and Progress. Am Psychol. 2014.
- Vowles KE, McCracken LM. Acceptance and valuesbased action in chronic pain: a study of treatment effectiveness and process. J Consult Clin Psychol. 2008;76(3):397-407. doi:10.1037/0022-006X.76.3.397.
- Cherkin DC, Sherman KJ, Balderson BH, et al. Effect of Mindfulness-Based Stress Reduction vs Cognitive Behavioral Therapy or Usual Care on Back Pain and Functional Limitations in Adults With Chronic Low Back Pain: A Randomized Clinical Trial. JAMA. 2016; 315(12): 1240-1249.
- Zeidan F, Vago DR. Mindfulness meditation-based pain relief: a mechanistic account. Ann N Y Acad Sci. 2016;1373(1):114-127. doi:10.1111/nyas.13153.
- Hilton L, Hempel S, Ewing BA, et al. Mindfulness Meditation for Chronic Pain: Systematic Review and Meta-analysis. Ann Behav Med Publ Soc Behav Med. 2017;51(2):199-213.
- Pradhan EK, Baumgarten M, Langenberg P, et al. Effect of Mindfulness-Based Stress Reduction in rheumatoid arthritis patients. Arthritis Rheum. 2007;57(7):1134-1142. doi:10.1002/art.23010
- Anheyer D, Haller H, Barth J, Lauche R, Dobos G, Cramer H. Mindfulness-Based Stress Reduction for Treating Low Back Pain: A Systematic Review and Meta-analysis. Ann Intern Med. 2017;166(11): 799-807. doi:10.7326/M16-1997.
- Carlson LE, Garland SN. Impact of mindfulness-based stress reduction (MBSR) on sleep, mood, stress and fatigue symptoms in cancer outpatients. Int J Behav Med. 2005;12(4):278-285. doi:10.1207/s15327558ijbm1204_9.
- Grossman P, Niemann L, Schmidt S, Walach H. Mindfulness-based stress reduction and health benefits. A meta-analysis. J Psychosom Res. 2004;57(1):35-43. doi:10.1016/S0022-3999(03)00573-7
- Omidi A, Zargar F. Effects of mindfulness-based stress reduction on perceived stress and psychological health in patients with tension headache. J Res Med Sci Off J Isfahan Univ Med Sci. 2015;20(11):1058-1063.
- Burger AJ, Lumley MA, Carty JN, et al. The effects of a novel psychological attribution and emotional awareness and expression therapy for chronic musculoskeletal pain: A preliminary, uncontrolled trial. J Psychosom Res. 2016;81:1-8.
- Neblett R. Surface Electromyographic (SEMG) Biofeedback for Chronic Low Back Pain. Healthcare. 2016;4(2).
- Nestoriuc Y, Martin A, Rief W, Andrasik F. Biofeedback treatment for headache disorders: a comprehensive efficacy review. Appl Psychophysiol Biofeedback. 2008;33(3):125-140.
- Elkins G, Jensen MP, Patterson DR. Hypnotherapy for the management of chronic pain. Int J Clin Exp Hypn. 2007;55(3):275-287.
- Kampman K, Jarvis M. American Society of Addiction Medicine (ASAM) National Practice Guideline for the Use of Medications in the Treatment of Addiction Involving Opioid Use. J Addict Med. 2015;9(5):358-367. Heyward J, Jones C, Compton W. Coverage of
- Nonpharmacologic Treatments for Low Back Pain Among US Public and Private Insurers. JAMA Netw Open. 2018;1(6). https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2705853.
- Kerns RD, Krebs EE, Atkins D. Making Integrated Multimodal Pain Care a Reality: A Path Forward. J Gen Intern Med. 2018;33(Suppl 1):1-3. doi:10.1007/s11606-018-4361-6.
- Heapy AA, Higgins DM, Goulet JL, et al. Interactive Voice Response–Based Self-management for Chronic Back Pain. JAMA Intern Med. 2017;177(6):765-773. doi:10.1001/jamainternmed.2017.0223.
- Roditi D, Robinson ME. The role of psychological interventions in the management of patients with chronic pain. Psychol Res Behav Manag. 2011;4:41-49. doi:10.2147/PRBM.S15375.
- Wahass SH. The Role of Psychologists in Health Care Delivery. J Fam Community Med. 2005;12(2):63-70.
- Darnall BD, Scheman J, Davin S, et al. Pain Psychology: A Global Needs Assessment and National Call to Action. Pain Med Malden Mass. 2016;17(2):250-263. doi:10.1093/pm/pnv095.
- Wandner LD, Prasad R, Ramezani A, Malcore SA, Kerns RD. Core competencies for the emerging specialty of pain psychology. Am Psychol. August 2018. doi:10.1037/amp0000330.
- Becker WC, DeBar LL, Heapy AA, et al. A Research Agenda for Advancing Non-pharmacological Management of Chronic Musculoskeletal Pain: Findings from a VHA State-of-the-art Conference. J Gen Intern Med. 2018;33(Suppl 1):11-15. doi:10.1007/s11606-018-4345-6.
No comments:
Post a Comment