Ulnar Impaction Syndrome
Dr. KS Dhillon
Introduction
Ulnar impaction syndrome is a degenerative condition of the wrist caused by the impaction of the ulnar head on the ulnar-sided carpal bones. This abutment causes an increase in load bearing across the ulnar head, triangular fibrocartilage complex (TFCC), and ulnar carpals. This increased loading causes degeneration of the TFCC, chondromalacia of the ulna and carpals, especially the lunate, and disruption of the triquetrolunate ligament [1]. This condition is also known as ulnar abutment or ulnocarpal loading.
The most common predisposing factor is positive ulnar variance where there is an increased ulnar length relative to the radius. In the positive ulnar variance wrist, the TFCC is stretched and is thin, and greater biomechanical forces, specially rotation forces, impact the joint.
Positive variance can be congenital [1] or acquired [2] radial shortening secondary to trauma. Radial shorting can be due to a malunion of the radius after a distal radius fracture, an Essex-Lopresti injury, proximal migration of the radius after radial head excision, or premature physeal closure of the radius
[1-3].
Wrists that do not have positive ulnar variance can also acquire ulna impaction syndrome because variance can increase during functional activities, such as forearm pronation and gripping [3,4]. When ulnar variance increases in wrists that are ulnar negative or neutral ulnocarpal load also increases [5]. Hence, although ulna impaction syndrome is most common in those with an ulnar-positive wrist, it can also occur in wrists with either negative or neutral variance [4].
Ulnar impaction syndrome is insidious and progressive. Patients can be asymptomatic and have the syndrome or they can be severely symptomatic. Symptomatic patients present with wrist pain. Examination shows occasional edema, decreased range of wrist movements, decreased forearm rotation, and tenderness to palpation dorsally just distal to the ulnar head and just volar to the ulnar styloid process. Forceful grip, forearm pronation, and ulnar deviation usually aggravates the pain [5].
Radiologic evaluations including magnetic resonance imaging (MRI) are frequently performed for patients with ulna impaction syndrome. The MRI allows for earlier detection of an abnormality in the TFCC, cartilage, and bone marrow of carpal bones. It is also useful for differential diagnosis of ulnar-sided wrist pain [6-8].
There is little information available to analyze unsatisfactory outcomes after conservative treatment for idiopathic ulna impaction syndrome. Knowledge of these factors will help physicians in predicting prognoses and help determine the proper indication for surgical treatment.
Etiology
In a normal neutral wrist, approximately 20% of the load goes to the ulna
and 80% goes to the radius. In a wrist with +2 mm, ulnar variance about 40% of the load goes to the ulna 60% goes to the radius.
Positive ulnar variance can be seen in patients with scapholunate dissociation, TFCC tears, lunotriquetral ligament tears, and radial shortening from previous distal radius fracture.
Clinical Presentation
Symptomatic patients present with ulna-sided wrist pain. The pain is on the dorsal side of DRUJ. The pain increases with ulnar deviation of the wrist and axial loading.
The following test can be done to diagnose ulna impaction syndrome:
1. Ballottement test
A dorsal and palmar displacement of the ulna with the wrist in ulnar deviation is done. The test is positive if the test produces pain.
2. Nakamura's ulnar stress test
Ulnar deviation of the pronated wrist while axially loading, flexing, and extending the wrist is carried out. A positive test produces pain.
3. Fovea test
The fovea test is used to evaluate for TFCC tear or ulnotriquetral ligament tear. It is performed by palpation of the ulnar wrist between the styloid and FCU tendon. The test is positive if there is tenderness.
Imaging
Radiographs
An AP radiograph with the wrist in neutral supination/pronation and zero rotation is taken to evaluate ulnar variance. A pronated grip view will show
increase in radiographic impaction.
Ulnar variance may be (fig 1 and 2):
neutral (both the ulnar and radial articular surfaces at the same level)
positive (ulna projects more distally)
negative (ulna projects more proximally)
The variance is independent of the length of the ulnar styloid process.
The normal variance is 0.9 mm with a range from -4.2 to +2.3 mm.
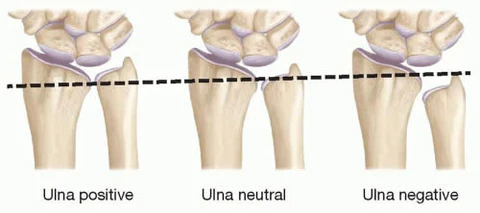
Fig 1

Fig 2
In patients with impaction syndrome, there will be ulna-positive variance and sclerosis of the lunate and ulnar head.
Arthrography of the wrist can show TFCC and lunotriquetral ligament tears.
An MRI of the wrist can be done to look for TFCC tears which can be caused by ulnocarpal impingement.
Differential diagnosis
The differential diagnosis for ulna impaction syndrome includes the following:
Ulnar styloid impaction syndrome. Ulnar styloid impaction syndrome causes ulnar-sided wrist pain secondary to impaction between the ulnar styloid tip and the triquetrum. The x-rays will show ulnar variance with subchondral sclerosis of the ulnar styloid and/or triquetrum.
DRUJ instability or arthritis. DRUJ instability and DRUJ arthritis can produce ulna-sided wrist pain.
TFCC tear. TFCC tear is a common cause of ulnar-sided wrist pain. The tear can result from trauma or due to degenerative changes.
Lunotriquetral (LT) ligament tear. LT ligament tears are rare traumatic injuries to the wrist that can lead to volar intercalated segment instability which is caused by a combination of injury to the lunotriquetral ligament and the dorsal radiocarpal ligament. X-rays will show volar flexion of the lunate.
Pisotriquetral arthritis. Degenerative arthritis of the pisotriquetral joint is diagnosed by point tenderness over the pisiform and crepitus elicited by lateral movement of the pisiform on the triquetrum.
Extensor carpi ulnaris (ECU) tendonitis or instability. Also known as snapping ECU. On palpation of the ECU tendon, there is a painful snap while moving the wrist from pronation to supination.
Lunotriquetral coalition. A normal variant that may rarely cause ulna-sided wrist pain.
Treatment
The first line of treatment is conservative. It includes immobilization of the wrist for 6 to 12 weeks, nonsteroidal anti-inflammatory drugs, corticosteroid injection, and limiting aggravating movements such as pronation, gripping, and ulnar deviation [5].
The operative options include:
A. Ulnar shortening osteotomy, [2,9] where the ulna is shortened, with removal of 2 to 3 mm of the shaft, and the ulna is fixed with a compression plate.
B. Arthroscopic wafer procedure,[10] where 2 to 4 mm of cartilage and bone is removed from under the TFCC arthroscopically. It is indicated if there is no lunotriquetral instability with minimal ulnar variance, cystic changes of carpus on radiographs, and evidence of degeneration of TFCC on magnetic resonance imaging.
C. Bowers procedure, [8] which involves resection of the ulnar articular head, leaving shaft and styloid relationship intact.
D. Darrach procedure,[8] where the ulnar head is excised if TFCC cannot be reconstructed;
E. Sauve-Kapandji procedure,[8] where resection of distal ulna and fusion of ulnar head and radius with a screw is done. This is a good option for manual laborers
F. Ulnar head replacement for severe ulnocarpal arthrosis and as a salvage procedure for failed Darrach.
There are several studies that have reported a high percentage of success with ulnar shortening osteotomy. Baek et al [2] showed significant improvements in patients with idiopathic impaction syndrome, where the postoperative modified Gartland and Werley scores improved significantly from the preoperative score. There was also reduced subluxation of the distal radioulnar joint, resolution of degenerative cystic changes of ulnar carpal bones, as well as a reduction in average ulnar variance from +4.6 preoperatively to −0.07 postoperatively.
Chun et al [9] showed 100% union in 6 to 8 weeks, and 72% excellent results on Gartland and Werley score.
In arthroscopic wafer procedure, [10] 85% to 100% of patients showed good to excellent results with a nearly full range of motion. The grip strength, however, did not improve and patients with a history of distal radius fracture had increased pain after surgery. Feldon et al [12] reported 69% excellent and 31% good results for open wafer procedure although it required longer postoperative immobilization and recovery. Tomanino et al, [4] using combined arthroscopic TFCC debridement and wafer resection, reported total pain relief in 67% of patients along with a 36% increase in grip strength.
References
Katz DI, Seiler JG, Bond TC. The treatment of ulnar impaction syndrome: a systematic review of the literature. J Surg Orth Adv. 2010;19(4):218-22.
Baek G, Chung M, Lee Y, Gong H, Lee S, Kim H. Ulnar shortening osteotomy in idiopathic ulnar impaction syndrome: surgical technique. J Bone Joint Surg Am. 2006;88 (suppl 1, pt 2):212-20.
Sachar K. Ulnar-sided wrist pain: evaluation and treatment of triangular fibrocartilage complex tears, ulnocarpal impaction syndrome, and lunotriquetral ligament tears. J Hand Surg Am. 2008;33:1669–1679. doi: 10.1016/j.jhsa.2008.08.026.
Tomaino MM, Elfar J. Ulnar impaction syndrome. Hand Clin. 2005;21:567–575. doi: 10.1016/j.hcl.2005.08.011.
Sammer DM, Rizzo M. Ulnar impaction. Hand Clin. 2010;26:549-57.
Imaeda T, Nakamura R, Shionoya K, Makino N. Ulnar impaction syndrome: MR imaging findings. Radiology. 1996;201:495–500. doi: 10.1148/radiology.201.2.8888248.
Ersoy H, Pomeranz SJP. Classification and Magnetic Resonance Imaging Findings of Ulnocarpal Impingement. J Surg Orthop Adv. 2015;24:257–262.
Cerezal L, et al. Imaging findings in ulnar-sided wrist impaction syndromes. Radiographics. 2002;22:105–121. doi: 10. 1148/radiographics.22.1.g02ja01105.
Chun S, Palmer AK. The ulnar impaction syndrome: follow-up of ulnar shortening osteotomy. J Hand Surg. 1993;24:316-20.
Meftah M, Keefer EP, Panagopoulos G, Yang SS. Arthroscopic wafer resection for ulnar impaction syndrome: prediction of outcomes. J Hand Surg. 2010;15(2):89-93.
Duke Orthopaedics: Wheeless’ Textbook of Orthopaedics Web site. Available at: http://www. whellessonline.com/ortho/. Accessed November 5, 2011.
Feldon P, Terrono AL, Belsky MR. The “wafer” procedure. Partial distal ulnar resection. Clin Orthop Relat Res. 1992, 275: 124–9.
No comments:
Post a Comment