Calcaneus Fractures
Dr. KS Dhillon
Introduction
Fractures of the calcaneus are rare but potentially debilitating injuries. The calcaneus bone is one of seven tarsal bones and it forms part of the hindfoot which includes the calcaneus and the talus. The hindfoot articulates with the fibula and tibia creating the ankle joint. The subtalar or talocalcaneal joint contributes to some foot and ankle plantar/dorsal flexion. Historically a burst fracture of the calcaneus was coined as a "Lovers Fracture" as the injury would occur as a suitor would jump off a lover's balcony to avoid detection [1-3].
Etiology
Calcaneal fractures most commonly occur when there is axial loading of the bone but can occur with any injury to the foot and ankle [4,5]. Falls from height and automobile accidents are the usual cause of the injury, although jumping onto hard surfaces, blunt or penetrating trauma, and twisting and shearing events can also cause the injury. Most of the injuries cause the bone to flatten, shorten and widen. Stress fractures can occur with overuse or repetitive use, such as running.
Epidemiology
Tarsal fractures account for 2% of all fractures. Calcaneal fractures account for 50-60% of all tarsal bone fractures. Less than 10% of the calcaneal fractures present as open fractures. Most of the injuries are industrial injuries, hence, traditionally, there is a male predominance. Most patients with calcaneus fractures are young, with the 20-39 age group being the most common. Comorbidities such as osteoporosis and diabetes may increase the risk of all types of fractures. Calcaneal fractures are rare in children.
Pathophysiology
Falls from a height translate energy directly into the calcaneus on impact as the heel strikes a surface. This causes crushing of the calcaneus against the talus. The talus acts as a wedge and causes depression and the widening of the calcaneal body [6,7]. During high-speed automobile accidents, a foot pressed against an accelerator, brake, or floorboard can translate a large amount of force through the calcaneus. Gunshot wounds and other ballistic injuries cause a more diffuse nonpredictable fracture pattern. The tibial nerve and artery run along the medial aspect of the calcaneum and are thought to be shielded by the sustentaculum tali thus neurovascular injuries are uncommon with calcaneal fractures.
History and Physical Examination
A traumatic event always precedes the presentation of calcaneal injury.
Patients will present with diffuse pain, edema, and ecchymosis at the fracture site. The patient is usually not able to bear weight on the affected limb. Plantar ecchymosis extending through the plantar arch of the foot is usually present. Associated disability of the Achilles tendon is often present. In patients with Tongue-type calcaneus fractures skin tenting may be present.
Evaluation
A complete neurovascular examination as well as evaluation of all lower extremity tendon function is carried out. A loss of ipsilateral dorsalis pedis or posterior tibial pulse should raise suspicion of arterial injury and prompt further investigation with angiography.
Initial bony evaluation is carried out with AP, lateral, and oblique plain films of the foot and ankle. A Harris view can be obtained which demonstrates the calcaneus in an axial orientation [8].
Computed tomography remains the gold standard for the diagnosis of calcaneal injuries. CT scan is used for preoperative planning and classification of fracture severity. It is useful for diagnosis when the plain X-rays are normal.
Mondor's Sign is a hematoma seen on a CT scan that extends along the sole and is considered pathognomic for calcaneal fracture. Stress fractures would be best evaluated with a bone scan or MRI.
Radiographs may show a depressed Bohler's Angle (fig 1). It is the angle between two lines drawn on plain film. The first line is between the highest point on the tuberosity and the highest point of the posterior facet and the second is the highest point on the anterior process and the highest point on the posterior facet. The normal angle is between 20-40 degrees.
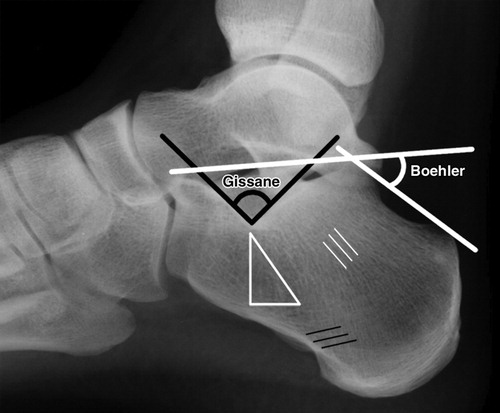
Fig 1.
An increase in the Critical Angle of Gissane (fig 1) may be seen. It is the angle between two lines drawn on plain film. The first is along the anterior downward slope of the calcaneus and the second is along the superior upward slope. The normal angle is between 130-145 degrees.
Normal Bohlers and Gissane angles, however, do not rule out a fracture.
Abnormal findings should prompt a CT scan for further classification and evaluation of the fracture.
There are two general categories of calcaneal fractures [9] [10]. The extraarticular fractures account for 25 % of calcaneal fractures. These are usually avulsion injuries of either the calcaneal tuberosity from the Achilles tendon, the anterior process from the bifurcate ligament, or the sustentaculum tali.
The intraarticular fractures account for the remaining 75% of the fractures. The talus acts as a wedge or hammer compressing the calcaneus at the angle of Gissane causing the fracture.
There are two main classification systems of extraarticular fractures of the calcaneum.
1. Essex-Lopresti:
There are two types of extraarticular fractures (fig 2). One is the joint depression type with a single verticle fracture line through the angle of Gissane separating the anterior and posterior portions of the calcaneus. The other is the tongue type which has the same verticle fracture line as a depression type with another horizontal fracture line running posteriorly, creating a superior posterior fragment. The tuberosity fragment may then rotate superiorly.
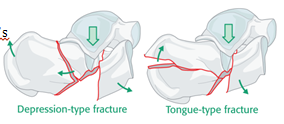
Fig 2.
2. Sanders Classification (fig3): This is based on reconstituted CT findings.
Type I fractures: There is 1 nondisplaced or minimally displaced bony fragment.
Type II fractures: There are 2 bony fragments involving the posterior facet. Type II is subdivided into types A, B, and C depending on the medial or lateral location of the fracture line.
Type III fractures: There are 3 bony fragments including an additional depressed middle fragment. Subdivided into types AB, AC, and BC, depending on the position and location of the fracture lines.
Type IV fractures: There are 4 comminuted bony fragments.

Fig 3.
Treatment
For contaminated wounds, aggressive wound care is carried out, and antibiotics are given [11]. Analgesics are given for pain. Ice is applied and the foot is elevated. Splinting of the fracture is done. They ambulate non-weight bearing.
Most extraarticular fractures are treated conservatively with 10-12 weeks of casting. Displaced calcaneal tuberosity and sustentaculum tali avulsion fractures and large substantial calcaneal body fractures may require surgery. Displaced intraarticular fractures are treated surgically. Surgery involves open reduction and internal fixation, percutaneous pinning, or sometimes arthrodesis. Undisplaced Sanders type I fractures can be treated conservatively.
A recent randomized controlled trial by Griffin et al [12] reviewed operative versus non-operative treatment for closed, displaced, intra-articular calcaneus fractures. The study included a total of 151 patients with 73 in the operative arm and 78 in the non-operative arm. The operative group was treated with the extensile lateral approach and the non-operative group was treated with initial immobilization followed by gentle mobilization as allowed by pain. There were complications in the operative group. There was infection and the hardware had to be removed in 11% of the operative group. However, there were no differences between the group with regards to health outcomes, range of motion, heel width, walking speed, and gait. All participants recovered very slowly from injury, most improvements plateaued at 18 months and most participants reported ongoing adverse effects from their injury at 2 years. The study concluded with recommendations against operative intervention for closed, displaced, intra-articular fractures of the calcaneus.
A more recent meta-analysis from 2017 by Wei et al [13] composed of 18 trials including 1467 patients found significantly improved anatomical improvements with operative intervention with regards to the restoration of Bohler's angle, calcaneal height, and width as well as the likelihood of resuming former work. There was a higher complication rate with operative treatment. The meta-analysis concluded that operative treatment of displaced, intra-articular calcaneal fractures have better anatomic recovery, functional outcomes, and return to work rate.
The aim of surgical management is to restore calcaneal morphology and to restore articular congruency. Operative intervention for calcaneal fractures is fraught with complications, hence the decision to move forward with surgery must be based on fully informed consent of the abundant risks and expected benefits of surgery.
Surgical treatment must be delayed until the soft tissue swelling subsides which can take upto 21 days [14]. Furthermore, all serous and hemorrhagic blisters must be epithelialized [8].
Surgical intervention is usually recommended for the following indications: [15]
Displaced tongue-type fractures
Joint depression with articular comminution or anterior process involvement
Bohler's angle of <5 degrees on initial presentation
Fracture dislocation
Anterior process fractures with >25% of the calcaneocuboid articulation involved
Calcaneal body fractures with significant varus or valgus malalignment, lateral impingement, loss of calcaneal height, or significant translation of the posterior tuberosity.
Open calcaneal fractures require emergency treatment with wound irrigation and debridement. The clinical outcomes with open calcaneal fractures are generally poorer than closed fractures. A study by Aldridge et al [16] in 2004 found that despite an increase in complication rates following treatment of open calcaneal fracture the quality of life metrics was higher than expected. They found that the complication rate was not as high as had been previously reported in the literature. They did recommend that definitive fixation should not be performed at the time of initial irrigation and debridement.
A study by Siebert et al [17] of 35 patients with 36 open calcaneal fractures showed that there were 23 cases with complications including the need for soft tissue coverage, nine cases of osteomyelitis, five amputations, and one arthrodesis. Their cohort of patients had poor quality of life metrics post-operatively. The worst outcome was seen in patients with Grade III open fractures.
Two approaches are available for the treatment of calcaneal fractures i.e the open extensile lateral approach, and the minimally invasive technique. Tourniquet is used for both approaches.
The extensile lateral approach has been the main approach for many years for the operative treatment of calcaneal fractures. It provides adequate visualization intra-operatively and allows for manipulation of the fracture to restore alignment and restore the articular surfaces. The extensile lateral approach is performed by creating full-thickness soft tissue and periosteal flaps as previously described by Gould and later modified by Benirschke and Sangeorzan [18]. The lateral calcaneus and joint surfaces can be well visualized and temporary retraction is created by the placement of Kirschner wires into the talus, fibula, and cuboid.
The fracture lines are opened and may include temporary removal of the lateral wall. Manual traction is used to restore the height and length of the tuberosity. Placement of a Steinmann pin into the tuberosity is helpful in restoring these parameters. The varus deformity must also be corrected. A temporary reduction can be maintained by the placement of Kirschner wires through the tuberosity fragment into the fragment of the medial sustentaculum. The lateral posterior facet joint surface must be anatomically reduced under direct visualization and may be held in place with lag screw fixation. Care must be taken to make sure that one does not over-penetrate the medial cortex. Overpenetration of the medial cortex may lead to entrapment of the flexor hallucis longus tendon. Reduction and alignment should be verified with fluoroscopy. The wound should be closed in layers after drain placement [14,18]. The closure is typically recommended with an interrupted Allgöwer-Donati stitch [19].
The goals of the minimally invasive technique (or sinus tarsi approach) are to minimize soft tissue injury while performing fracture reduction and stabilization. This approach is used for Sanders type II and III fractures. It is used in patients with comorbidities that make soft tissue more vulnerable to complications including diabetes mellitus, smoking, obesity, and peripheral vascular disease. The sinus tarsi approach is performed by creating a 2-4cm incision along a line from the tip of the fibula towards the base of the fourth metatarsal. That will allow direct visualization of the posterior facet and the anterolateral fragment of the lateral wall. Typically a small, low-profile plate is used for fixation after reduction of the joint surface. Adjunctive percutaneous screws are often placed to assist with the other parameters of calcaneal morphology. Alignment is assessed under fluoroscopy. This same incision may be used for subsequent subtalar arthrodesis should that be necessary [20].
Some authors are of the opinion that anatomic reduction, fracture disimpaction, and repositioning are exceedingly difficult with limited exposures. Once the surgeon has committed to the minimal approach conversion to the extensile lateral approach is not recommended. Great care must be taken in determining the correct approach for the correct patient [14]. A recent meta-analysis was performed comparing minimally invasive techniques with the standard lateral extensile approach. In this analysis, there were 2179 participants followed for an average of 22.41 months. The results of the analysis showed no statistically significant difference in post-operative calcaneal length, width, deep infection, or Gissane's angle between the two approaches. There was, however, a difference between wound complications, nerve injury, superficial infection, VAS pain scores, American Academy of Orthopedic Foot and Ankle Society (AOFAS) scores, calcaneal height, and post-operative Bohler's angle in favor of minimally invasive techniques. This is part of the growing body of evidence that the smaller incision techniques may be useful in certain groups [21]. Many authors contend that fractures with more severe patterns require the extensile approach and are also predisposed to a higher complication rate.
Kline et al [22] retrospectively reviewed a cohort of 112 calcaneal fractures of which 79 underwent the traditional extensile lateral approach and 33 were treated using minimally invasive techniques. The demographics of the two groups were comparable. The extensile group's fracture composition was 47% Sanders III and 53% Sanders II. The minimally invasive group's fracture composition was 39% Sanders III and 61% Sanders II. Both groups had a 100% union rate and similar radiographic parameters with regards to the angle of Gissane and Bohler's angle. The wound complication rate was 29% in the extensile lateral group with 9% of the treated cases requiring repeat surgery for those complications. Only 6% of the minimally invasive group had wound complications and none required additional surgery. Kline et al concluded that the minimally invasive technique was valuable and could lead to a lower complication rate and comparable clinical results [22]. Many other groups have found similar findings in the sinus tarsi approach. This approach seems to lead to similar radiographic and functional outcomes with fewer wound complications overall [23].
To mitigate the issue of soft tissue compromise some authors have adopted a two-stage surgical approach for severely displaced closed calcaneal fractures. The calcaneus becomes shortened and widened with heel varus as a result of the fracture displacement and loss of Bohler's angle.
Githens et al [15] used a medial external fixator to treat 21 fractures. They found that calcaneal length, height, and axial alignment can be restored with an external fixator. They also found that the Bohler's angle cannot be restored with an external fixator and ligamentotaxis alone. They had no deep or superficial wound infections requiring surgical intervention.
With tongue-type fractures, there can be variable amounts of displacement of the tuberosity fragment. Due to the pull of the Achilles tendon, significant superior and dorsal displacement can occur leading to the potential to tent the posterior heel skin and place the soft tissue at significant risk of breakdown. Urgent fracture reduction should be carried out at the first sign of skin compromise [24]. Gardner et al [24] in a series of 139 tongue-type fractures found 21% soft tissue compromise. Fractures with greater initial displacement were at a greater risk of skin compromise. None of the patients with identified threatened soft tissue upon presentation who were treated with emergent operative reduction and fixation went on to further soft-tissue complications [24].
For extremely comminuted fractures some surgeons will favor primary subtalar arthrodesis as it seems to reduce the need for subsequent procedures and the associated increased costs and lost time from work associated with those additional surgeries [25]. However, there are other studies that have found that patients who develop post-traumatic arthritis who first undergo open reduction internal fixation of their fractures with the intraoperative restoration of calcaneal morphology do better than those who develop subtalar arthritis due to malunion following non-operative treatment [26].
Prognosis
The Sanders classification has been found to have consistent prognostic value. One hundred and eight type II and III calcaneus fractures operatively treated were evaluated at a minimum of 10 years with an average follow-up time of 15.22 years. CT scan was performed immediately postoperatively and 95% of the fractures had posterior facet reduction to the anatomic position with no appreciable step-off of the articular surface and with no reductions more than 5mm inaccurately reduced. The results of this cohort of verifiably well-reduced fractures demonstrated that type III fractures were 4 times more likely to require eventual subtalar fusion compared to type II fractures. The long-term functional results in this cohort resulted in mild pain and some alterations in activities of daily living [14].
Certain populations tend to have better results [27]:
Women
Younger Adults
Patients with a lighter workload (office work compared to heavy manual labor employment)
Patients not receiving workers compensation
Patients with a higher initial Bohler's angle. The amount of initial displacement based on Bohler's angle of less than 0 degrees is correlated with lower functional outcomes. When the initial Bohler's angle is greater than fifteen degrees upon presentation their functional results will be better regardless of operative versus non-operative treatment [8].
Complications
Concomitant injuries must be considered due to the fact that severe force is required to sustain calcaneal fractures [28][29]. Greater than 70% of patients with calcaneus fractures have additional injuries.
A thorough examination of the entire spine is performed whenever a calcaneal fracture is identified especially when a fall is the cause. The force from impacting the ground passes through the lower extremity and upward sometimes causing spinal compression fractures.
Compartment syndrome of the foot is rare. It can occur in up to 10% of the injuries. A high index of suspicion is needed in patients presenting with increased pain either after treatment or during the initial evaluation.
Postoperative wound infection, osteomyelitis, malunion, and subtalar arthritis are all potential complications of calcaneal fractures.
Wound breakdown and infections are the most common and devastating complications of the extensile lateral approach. Wound complications and infections can be as high as 37% and 20% respectively following operative intervention [20].
Subtalar osteoarthritis can result from surgical or nonsurgical treatment. It is more common with non-operatively treated displaced intra-articular calcaneus fractures. Subtalar fusion may be required for subtalar arthritis [8]. Another study [30] found that non-operative measures were up to 6 times more likely to lead to late subtalar fusion due to symptomatic subtalar arthritis.
Sural nerve injury can occur in up to 15% of cases treated operatively via the extensile lateral approach. The risk is reduced with an inferiorly based L-incision [31].
Chronic pain is also a common complication in many cases due to post-traumatic subtalar arthritis, malalignment, or stiffness resulting from the injury.
Peroneal tendon instability can result from displaced, intra-articular calcaneus fractures [32]. This can result from direct damage to the tendons themselves as a result of the injury or fracture fragments that may impinge on the tendons. Up to a 40% displacement of the peroneal tendons has been seen on CT scans of calcaneus fractures [33]. With significant height loss, calcaneal widening, and hindfoot varus, subfibular impingement may result from soft tissue or osseous abnormalities. Subfibular impingement may result in lateral heel pain, especially with eversion of the hindfoot. Techniques have been described to perform percutaneous calcaneal osteotomy and peroneal tendon decompression to alleviate subfibular impingement after calcaneal malunion [34].
Postoperative Care
Following the surgery, the patient's foot and ankle are placed into an extremely well-padded posterior splint. Drains are usually removed on postoperative day two.
The patient should be advised to elevate the extremity for the first several weeks after surgery to reduce swelling. The splint may be removed as early as 2-5 days or left in place for 2 weeks in some cases. After removing the splint the patient should begin range of motion exercises for the subtalar and ankle joint.
Weight-bearing is usually delayed 8-12 weeks or more depending on the degree of comminution and progression of healing on radiographs. Routine serial radiographs are taken to monitor the progression of healing.
Conclusion
Fractures of the calcaneus are rare but potentially debilitating injuries.
A good history is taken and a full neurovascular and musculoskeletal examination is carried out when a calcaneal fracture is suspected. Correct diagnosis and workup must include X-Rays, and a CT scan is considered the gold standard for making a diagnosis.
Consideration must also be given to imaging other parts of the patient's body to exclude other fractures.
Initial splinting, ice, and elevation of the limb will be useful to help improve tissue quality for later operative intervention.
Patients have to be told about the advantages and disadvantages of surgical treatment.
Once the patient and the surgeon have decided to proceed with surgical treatment the aim must include adequate reduction of articular surfaces and restoration of calcaneal morphology.
The patient has to be counseled of the expected sequela of surgical treatment and that, despite an adequate reduction, in severe injuries subtalar osteoarthritis is common.
Overall the outlook for patients with calcaneus fractures is rather guarded. Patients with isolated fractures do recover with time but those with concomitant injury to the pelvis, spine, neck, or head often require prolonged rehabilitation and can have residual physical deficits.
Displaced type III fractures have a higher likelihood of leading to subtalar arthrodesis than lower classification injuries.
Complete recovery from a calcaneus fracture can take months or even years [35,36].
References
Adams MR, Koury KL, Mistry JB, Braaksma W, Hwang JS, Firoozabadi R. Plantar Medial Avulsion Fragment Associated With Tongue-Type Calcaneus Fractures. Foot Ankle Int. 2019 Jun;40(6): 634-640.
Bibbo C, Siddiqui N, Fink J, Powers J, Ehrlich DA, Kovach SJ. Wound Coverage Options for Soft Tissue Defects Following Calcaneal Fracture Management (Operative/Surgical). Clin Podiatr Med Surg. 2019 Apr;36(2):323-337.
Cottom JM, Douthett SM, McConnell KK. Intraoperative Reduction Techniques for Surgical Management of Displaced Intra-Articular Calcaneal Fractures. Clin Podiatr Med Surg. 2019 Apr;36(2):269-277.
Hordyk PJ, Fuerbringer BA, Roukis TS. Clinical Management of Acute, Closed Displaced Intra-Articular Calcaneal Fractures. Clin Podiatr Med Surg. 2019 Apr;36(2):163-171.
Schepers T. Sinus Tarsi Approach with Screws-Only Fixation for Displaced Intra-Articular Calcaneal Fractures. Clin Podiatr Med Surg. 2019 Apr;36(2):211-224.
Herrera-Pérez M, Oller-Boix A, Valderrabano V, González-Casamayor S, Gutiérrez-Morales MJ, Guerra-Ferraz A, País-Brito JL. [Calcaneal fractures: controversies and consensus]. Acta Ortop Mex. 2018 May-Jun;32(3):172-181.
Diacon AL, Kimmel LA, Hau RC, Gabbe BJ, Edwards ER. Outcomes of midfoot and hindfoot fractures in multitrauma patients. Injury. 2019 Feb;50(2):558-563.
Buckley RE, Tough S. Displaced intra-articular calcaneal fractures. J Am Acad Orthop Surg. 2004 May-Jun;12(3):172-8.
Jiménez-Almonte JH, King JD, Luo TD, Aneja A, Moghadamian E. Classifications in Brief: Sanders Classification of Intraarticular Fractures of the Calcaneus. Clin Orthop Relat Res. 2019 Feb;477(2): 467-471.
Shih JT, Kuo CL, Yeh TT, Shen HC, Pan RY, Wu CC. Modified Essex-Lopresti procedure with percutaneous calcaneoplasty for comminuted intra-articular calcaneal fractures: a retrospective case analysis. BMC Musculoskelet Disord. 2018 Mar 09;19(1):77.
Sop JL, Sop A. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Aug 8, 2022. Open Fracture Management.
Griffin D, Parsons N, Shaw E, Kulikov Y, Hutchinson C, Thorogood M, Lamb SE., UK Heel Fracture Trial Investigators. Operative versus non-operative treatment for closed, displaced, intra-articular fractures of the calcaneus: randomised controlled trial. BMJ. 2014 Jul 24;349: g4483.
Wei N, Yuwen P, Liu W, Zhu Y, Chang W, Feng C, Chen W. Operative versus nonoperative treatment of displaced intra-articular calcaneal fractures: A meta-analysis of current evidence base. Medicine (Baltimore). 2017 Dec;96(49):e9027.
Sanders R, Vaupel ZM, Erdogan M, Downes K. Operative treatment of displaced intraarticular calcaneal fractures: long-term (10-20 Years) results in 108 fractures using a prognostic CT classification. J Orthop Trauma. 2014 Oct;28(10):551-63.
Githens M, Shatsky J, Agel J, Bransford RJ, Benirschke SK. Medial external fixation for staged treatment of closed calcaneus fractures: Surgical technique and case series. J Orthop Surg (Hong Kong). 2017 Sep-Dec;25(3):2309499017727915.
Aldridge JM 3rd, Easley M, Nunley JA. Open calcaneal fractures: results of operative treatment. J Orthop Trauma. 2004 Jan;18(1):7-11. doi: 10.1097/00005131-200401000-00002. PMID: 14676550.
Siebert CH, Hansen M, Wolter D. Follow-up evaluation of open intra-articular fractures of the calcaneus. Arch Orthop Trauma Surg. 1998;117(8):442-7. doi: 10.1007/s004020050289. PMID: 9801778.
Benirschke SK, Sangeorzan BJ. Extensive intraarticular fractures of the foot. Surgical management of calcaneal fractures. Clin Orthop Relat Res. 1993 Jul;(292):128-34.
Shannon SF, Houdek MT, Wyles CC, Yuan BJ, Cross WW, Cass JR, Sems SA. Allgöwer-Donati Versus Vertical Mattress Suture Technique Impact on Perfusion in Ankle Fracture Surgery: A Randomized Clinical Trial Using Intraoperative Angiography. J Orthop Trauma. 2017 Feb;31(2):97-102.
Hsu AR, Anderson RB, Cohen BE. Advances in Surgical Management of Intra-articular Calcaneus Fractures. J Am Acad Orthop Surg. 2015 Jul;23(7):399-407.
Seat A, Seat C. Lateral Extensile Approach Versus Minimal Incision Approach for Open Reduction and Internal Fixation of Displaced Intra-articular Calcaneal Fractures: A Meta-analysis. J Foot Ankle Surg. 2020 Mar-Apr;59(2):356-366.
Kline AJ, Anderson RB, Davis WH, Jones CP, Cohen BE. Minimally invasive technique versus an extensile lateral approach for intra-articular calcaneal fractures. Foot Ankle Int. 2013 Jun;34(6): 773-80.
Li LH, Guo YZ, Wang H, Sang QH, Zhang JZ, Liu Z, Sun TS. Less wound complications of a sinus tarsi approach compared to an extended lateral approach for the treatment of displaced intraarticular calcaneal fracture: A randomized clinical trial in 64 patients. Medicine (Baltimore). 2016 Sep;95(36):e4628.
Gardner MJ, Nork SE, Barei DP, Kramer PA, Sangeorzan BJ, Benirschke SK. Secondary soft tissue compromise in tongue-type calcaneus fractures. J Orthop Trauma. 2008 Aug;22(7):439-45.
Buckley R, Leighton R, Sanders D, Poon J, Coles CP, Stephen D, Paolucci EO. Open reduction and internal fixation compared with ORIF and primary subtalar arthrodesis for treatment of Sanders type IV calcaneal fractures: a randomized multicenter trial. J Orthop Trauma. 2014 Oct;28(10):577-83.
Radnay CS, Clare MP, Sanders RW. Subtalar fusion after displaced intra-articular calcaneal fractures: does initial operative treatment matter? Surgical technique. J Bone Joint Surg Am. 2010 Mar;92 Suppl 1 Pt 1:32-43.
Buckley R, Tough S, McCormack R, Pate G, Leighton R, Petrie D, Galpin R. Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: a prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am. 2002 Oct;84(10):1733-44.
Spierings KE, Min M, Nooijen LE, Swords MP, Schepers T. Managing the open calcaneal fracture: A systematic review. Foot Ankle Surg. 2019 Dec;25(6):707-713.
Zhang Z, Wang Z, Zhang Y, Qiu X, Chen Y. Risk factors for increased postoperative drainage of calcaneal fractures after open reduction and internal fixation: An observational study. Medicine (Baltimore). 2018 Aug;97(32):e11818.
Csizy M, Buckley R, Tough S, Leighton R, Smith J, McCormack R, Pate G, Petrie D, Galpin R. Displaced intra-articular calcaneal fractures: variables predicting late subtalar fusion. J Orthop Trauma. 2003 Feb;17(2):106-12.
Eastwood DM, Langkamer VG, Atkins RM. Intra-articular fractures of the calcaneum. Part II: Open reduction and internal fixation by the extended lateral transcalcaneal approach. J Bone Joint Surg Br. 1993 Mar;75(2):189-95.
Toussaint RJ, Lin D, Ehrlichman LK, Ellington JK, Strasser N, Kwon JY. Peroneal tendon displacement accompanying intra-articular calcaneal fractures. J Bone Joint Surg Am. 2014 Feb 19;96(4):310-5.
Ohashi K, Sanghvi T, El-Khoury GY, Ahn JM, Bennett DL, Geijer M, Inaoka T, Berbaum K. Diagnostic accuracy of 3D color volume-rendered CT images for peroneal tendon dislocation in patients with acute calcaneal fractures. Acta Radiol. 2015 Feb;56(2):
190-5.
Chu KM, Lui TH. Endoscopic Lateral Calcaneal Ostectomy and Peroneal Tendon Decompression With the Patient in the Prone Position as Management of Subfibular Impingement After Calcaneal Fracture. Arthrosc Tech. 2019 Oct;8(10):e1069-e1073.
Albin SR, Koppenhaver SL, Marcus R, Dibble L, Cornwall M, Fritz JM. Short-term Effects of Manual Therapy in Patients After Surgical Fixation of Ankle and/or Hindfoot Fracture: A Randomized Clinical Trial. J Orthop Sports Phys Ther. 2019 May;49(5):310-319.
Toro G, Langella F, Gison M, Toro G, Moretti A, Toro A, Iolascon G. Stentoplasty of calcaneal fractures: Surgical technique and early outcomes. Injury. 2019 Jul;50 Suppl 2:S70-S74.
No comments:
Post a Comment