Hallux Valgus
DR KS Dhillon
Introduction
Hallux valgus is also known as a bunion (fig 1). It is one of the most common forefoot deformities. Hallux valgus manifests with deviation of the proximal phalanx of the big toe laterally and the first metatarsal head medially. The first metatarsal head deviates medially due to adduction of the first metatarsus, called metatarsus primus varus. The precise etiology, however, is not fully understood. Hallux valgus tends to occur more commonly in women than in men, with a ratio as high as 15:1. It occurs more in those who wear tight shoes or heels [1].
Hallux valgus deformity can be diagnosed by physical examination. Imaging is useful to evaluate whether there is damage to the first metatarsophalangeal (MTP) joint. Treatment is initially conservative with the use of wider shoes, use of orthotics, and night splinting. If conservative treatment fails, surgical management is recommended. Patients usually tolerate the surgery well. Bony union usually occurs around 6 to 7 weeks postoperatively [1].
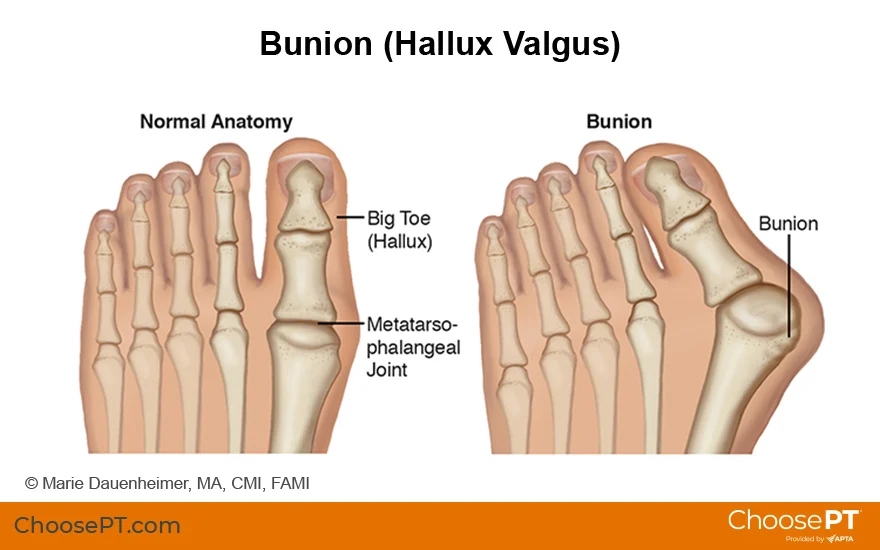
Fig 1.
Etiology
The exact etiology is not known. There are, however, many proposed theories. Hallux valgus deformity is most likely the result of multiple contributing factors such as genetics, short first metatarsal, flexible or rigid forefoot varus, rigid or flexible pes planovalgus, dorsiflexed first metatarsal, gastrocnemius equinus, abnormal foot mechanics, and joint hypermobility. Certain arthritic conditions such as gouty arthritis, psoriatic arthritis, and rheumatoid arthritis predispose patients to hallux valgus deformity. Furthermore, hallux valgus deformity is more commonly seen in connective tissue disorders such as Marfan syndrome, Ehlers-Danlos syndrome, and Down syndrome [2].
Muscle imbalance in the foot due to conditions such as cerebral palsy, stroke, or myelomeningocele can also cause a hallux valgus deformity.
Hallux valgus deformity is common in people who wear tight shoes and heels. Men who wear good footwear often have marked deformity, while women who wear footwear that compresses their feet have no deformity. This fact has led to the belief that footwear exacerbates an underlying bony abnormality rather than acting as the primary cause.
Epidemiology
Hallux valgus deformity is a common condition. It occurs in about 23% of adults aged 18 to 65 years and up to 36% of adults older than 65 years. Hallux valgus deformity occurs in about 30% of adult females [3]. The prevalence is higher in those who wear shoes or heels as compared to the barefoot population. When comparing women and men in the barefoot populations, women are found to have hallux valgus deformity twice as often.
Pathophysiology
The pathophysiology of hallux valgus is complex. The general assumption is that an imbalance exists between the extrinsic and intrinsic muscles of the foot. There is involvement of the ligaments as well. The first metatarsal alignment is created by the tension created by the peroneus longus laterally and the abductor hallucis muscle medially. The collateral ligaments prevent movement along the transverse plane at the first MTP joint. When there is increased pressure at the head of the first metatarsal, the metatarsal moves medial-dorsally. This increases the hallux angle, which is worsened by muscle stabilization while walking. When these forces push the first metatarsal medially and the hallux laterally, the medial collateral ligament and the medial capsule become strained and eventually rupture. Without stabilizing structures on the medial side, the lateral structures i.e. adductor hallucis muscle, collateral ligament, and lateral joint capsule, exacerbate this deformity [4].
History
Patients can present initially in several ways. The patient can present with a nonacute onset of deep or sharp pain to the first MTP joint during ambulation. The pain is exacerbated during particular activities. The patient may also describe aching pain in the metatarsal head secondary to shoe irritation. This pain is relieved when the shoes are removed. Usually, both forms of pain are progressive and have been present for many years. The frequency or duration of pain may recently have begun to increase. Patients may even describe a recent notable increase in the size of the deformity.
Questions about limitations of physical or daily living activities are useful for understanding the severity of the patient's pain. It is also important to ascertain what, if anything, relieves the pain.
Another possible presentation is burning pain or tingling in the dorsal aspect of the bunion. This indicates neuritis of the medial dorsal cutaneous nerve secondary to pressure either from the enlarged bone or the footwear. The patient may also describe symptoms caused by the deformity. This would include a painful overlapping second digit, interdigital keratosis, or ulceration on the medial metatarsal head.
Physical Examination
The physical examination includes a comprehensive assessment of the dermatologic, vascular, neurologic, and musculoskeletal systems.
The musculoskeletal assessment can be divided into two components. One is to determine the etiology and the other is the evaluation of the resultant pathology i.e. the presenting deformity.
The physical workup is tailored to the patient's history. If neurologic complaints, systemic arthritis, or collagen vascular disease were present, they should be addressed in more detail. If none of these are present, the focus then is on biomechanical examination. This includes the assessment of the following, any or all of which can contribute to hallux valgus:
Tibial torsion
Hip internal/external rotation
Genu valgum/varum
Ankle joint stiffness, especially decreased dorsiflexion
Subtalar joint stiffness
Midtarsal joint stiffness
Neutral calcaneal stance position
Resting calcaneal stance position
Forefoot/rearfoot varus or valgus
Assessment of resultant pathology can be divided into weight-bearing and non-weightbearing evaluations. Both can yield important information for determining the appropriate treatment protocol.
Nonweightbearing evaluation
The position of the hallux, with respect to the second digit, is assessed in the transverse plane. The hallux can be under-riding, overriding, abutting, or without contact. The lateral deviation of the MTP may be due to subluxation at the MTP joint. The medial prominence also requires evaluation.
The first MTP joint range of motion should undergo assessment for the maximum motion. The normal plantar flexion is less than 15 degrees and dorsiflexion is 65 to 75 degrees. Next, the quality of the first MTP joint is accessed for pain and crepitation. Finally, the MTP is evaluated for its axis of motion.
Weightbearing evaluation
The hallux valgus deformity tends to be more obvious when the patient is weight-bearing. When weight-bearing, the patient is evaluated for increased hallux abduction, increase in the medial prominence, first MTP joint dorsiflexion, hallux purchase, and metatarsus varus.
Evaluation
Usually, routine laboratory studies are not required. However, if there is suspicion of metabolic or systematic disease certain laboratory studies can be done. These include rheumatoid factor, erythrocyte sedimentation rate, uric acid, antinuclear antibody, c-reactive protein, and complete blood count. If there is suspicion of osteomyelitis, MRI and radionuclide imaging can be done.
The diagnosis can usually be established by physical examination. Imaging can help determine the extent of first MTP joint damage. Evaluation is done with plain radiography, with AP and lateral weight-bearing x-rays of the foot. Imaging will show a lateral hallux deviation at the first metatarsal. The normal hallux valgus angle is less than 15 degrees, and the intermetatarsal angle is less than 9 degrees. The deviation is in the transverse plane. Hallux valgus deformity can cause rotation of the hallux resulting in the nail facing medially.
The classification is mild, moderate, and severe based on the weight bearing anteroposterior, lateral oblique, lateral, and sesamoid axial views. The imaging helps to evaluate the structural status of the foot. The AP view helps to assess the intermetatarsal angle, hallux abductus angle, metatarsus adductus angle, hallux abductus interphalangeal, hallux rotation, and the condition of the first MTP joint. The lateral view primarily serves to assess the first metatarsal position (plantar-flexed or elevated) and dorsal exostosis/osteophytes. The lateral oblique projection helps evaluate the density, uniformity, and trabeculation of the bone stock. The sesamoid axial view looks primarily for sesamoid subluxations and degenerative joint changes.
Degree of hallux valgus: Hallux valgus angle (HVA) / Intermetatarsal angle (IMA)
Normal: less than15 degrees / 9 degrees
Mild: 15 to 30 degrees / 9 to 13 degrees
Moderate: 30 to 40 degrees / 13 to 20 degrees
Severe: over 40 degrees / over 20 degrees
Treatment
Treatment of patients with hallux valgus can be non-surgical or surgical. Non-surgical treatments are usually attempted first. If non-surgical treatment fails surgical repair is carried out. However, there is no definitive evidence that conservative treatment is effective. The American College of Foot and Ankle Surgeons recommends using conservative therapy before considering a surgical treatment. It is essential for patients to try wide shoes and orthotics before considering other more invasive options.
The aim of conservative treatment is to treat the symptoms without correcting the anatomical deformity. The non-surgical treatments options include:
Shoe modification: Low-heeled, wide shoes.
Ice: Icing the inflamed deformity to reduce inflammation.
Orthoses: Improves alignment and support.
Analgesics: Acetaminophen and NSAIDs.
Medial bunion pads: Prevents irritation of hallux valgus deformity.
Stretching: Helps maintain joint mobility in the affected joint.
If the non-surgical treatment is not able to control the pain, the treatment is deemed to have failed. At this point, surgical management is considered. Indication for surgery is primarily based on symptoms such as difficulty with ambulation, and pain. There are over 150 surgical procedures described for the correction of HV deformity. Some of the surgical procedures include:
Osteotomy
An osteotomy of the first metatarsal can be done to correct the deformity. A cut is made in the first metatarsal bone. The position of the cut and shape varies depending on the surgical strategy.
A Wilson osteotomy utilizes a straight cut, while the chevron osteotomy uses a wedge-shaped cut. The location of the cut may be near the base of the metatarsal (proximal osteotomy), in the shaft (scarf osteotomy), or in the neck (distal osteotomy).
A randomized control trial by Torkki et al [5] compared chevron osteotomy to no treatment or orthosis. They found that the chevron osteotomy outperformed the other treatment strategies. At 12 months follow-up, the hallux abductus angle was normal in the osteotomy group, with an 80% satisfaction rate. However, about 61% of the patients in the osteotomy group had moderate footwear problems. The surgery group required the greatest number of sick days and higher foot care costs. Most often, a distal metatarsal open approach is taken. There are newer minimally invasive techniques that are increasingly being used. A study that compared open osteotomy to minimally invasive surgery revealed no significant difference in the success of the surgery. However, the surgical time was reduced, and the scar was smaller in the minimally invasive surgery group. A randomized control trial comparing open versus minimally invasive chevron osteotomies found clinical and radiographic outcomes to be similar between the two treatment groups [6].
Arthroplasty
With an arthroplasty, the mobility of the first MTP joint is maintained while the pain is relieved. An excision arthroplasty or a joint replacement can be done. Both total joint arthroplasty and hemiarthroplasty have been developed. A hemiarthroplasty maintains toe length and requires less bone resection. An interposition arthroplasty is done in patients with severe hallux rigidus and it helps maintain joint range of motion. The most common arthroplasty is the Keller resection arthroplasty. In this procedure, about 50% of the proximal phalanx is resected to increase dorsiflexion and decompress the joint. With the Keller’s arthroplasty, 75% of patients are satisfied with the results, and 88% have complete pain relief. About 12% of patients experience increased pain [7].
Arthrodesis
When the MTP joint is severely degenerated and regaining function is unlikely an arthrodesis of the joint can be carried out [8]. The procedure is usually done in older patients. Postoperatively, up to 81% of patients have pain relief and improved ambulation. Nonunions have been found in up to 20% of the patients. Patients usually complain of limited footwear options, metatarsalgia, and joint stiffness. Fusion of the 1st metatarsal-cuneiform joint can also be done. It is usually reserved for patients with hypermobility of the 1st ray and severely increased hallux valgus and 1st intermetatarsal angles. More recently, the arthrodesis at this level has been modified to address the tri-planar deformity of hallux valgus. The results have been positive when assessing functional outcomes, diminished recurrence rates, and early return to weight-bearing activities [9].
Soft tissue procedures
The McBride procedure can also be used to treat hallux valgus. In this procedure, the fibular sesamoid is excised. This produces interphalangeal joint flexion, MTP joint hyperextension, and medial deviation of the hallux. There are no reports that have studied soft tissue procedures for hallux valgus deformity correction. One study compared chevron osteotomy alone to chevron plus adductor tenotomy. The study found little difference in mechanical correction and no difference in patient satisfaction [10].
There are very few randomized trials evaluating the efficacy of these surgical procedures. As surgical techniques have improved, patient satisfaction has also improved. Patient satisfaction ranges from 50 to 90%. Surgical outcomes, however, do not appear to correlate with patient satisfaction. This is believed to be related to the unmet postsurgical expectations of the patient.
Postoperative care depends on the type of procedure performed. The dressing is applied at the time of surgery to maintain corrective forces. The weight-bearing status depends on the procedure done. Usually, weight bearing is limited for the first two weeks. Once the sutures are removed, range of motion exercises and increasing weight-bearing activities are allowed.
Long-term monitoring is needed to understand the exact etiology to ensure the deformity does not recur. If the etiology is identified, the causes should be treated. Postsurgery patients may benefit from orthotic devices, notably in diseases that accelerate joint degeneration, such as rheumatoid arthritis.
Differential Diagnosis
The differential diagnosis of Hallux valgus deformity would include the following:
Osteoarthrosis
Freiberg disease
Gout
Septic joint
Hallux rigidus
Morton neuroma
Turf toe
Staging
Root et al [11] divided hallux valgus deformity into four stages:
Stage 1: There is lateral displacement of the hallux at the MTP joint
Stage 2: Progression of the hallux abduction where the hallux presses against the second toe.
Stage 3: Increased intermetatarsal angle, possible associated second hammertoe deformity.
Stage 4: Partial/Complete hallux dislocation at the MTP joint.
Prognosis
The prognosis of hallux valgus deformity is good. Patients are initially treated conservatively. If conservative treatment fails surgery is carried out. The postoperative recovery depends on the procedure carried out. Healing following the bony procedure takes around 6 to 7 weeks. If the patient is a smoker, the healing can take longer [12]. Patients usually return to work about 6 to 12 weeks post-surgery. Improvement can occur up to 1-year post-surgery [13].
Postsurgical complications depend on the surgical procedure carried out. They include osseous nonunion, cellulitis, avascular necrosis, hallux varus, limited joint range of motion, hematoma, numbness, hardware failure, osteomyelitis, and recurrence [14].
Recurrence rates differ based on the procedure done. It ranges from 10 to 47%. The etiology is multifactorial and includes anatomic predisposition, compliance with postsurgical instructions, medical comorbidities, and poor surgical technique [15].
Complications
Hallux valgus deformity can result in several complications. These include [16]:
Bursitis (most common)
Degenerative disease of the metatarsal head
Second toe hammertoe deformity
MTP joint synovitis
Central metatarsalgia
Medial dorsal cutaneous nerve entrapment
Conclusion
Hallux valgus deformity of the big toe is also known as a bunion. It is one of the common forefoot deformities. The big toe bends towards the other toes, and the joint can become red and painful. The exact cause is not known. It occurs more often in women and people who wear heels or tight shoes. The diagnosis is made by physical exam. Imaging helps to assess the severity of the deformity. The initial treatment is non-surgical with the use of wider shoes, use of orthotics, and night splinting. If this is not effective, surgical management is carried out. Patients typically tolerate the surgery well, and bony union usually occurs in about 6 to 7 weeks.
In smokers, the healing can take longer, and there is a higher risk of complications such as non-union or wound infection. Patients usually return to work approximately 6 to 12 weeks after surgery. Improvement can occur over a one-year period.
If surgery is performed, rehabilitation should follow. Patients are followed up over a long period to ensure they are meeting their recovery milestones.
References
Piqué-Vidal C, Solé MT, Antich J. Hallux valgus inheritance: pedigree research in 350 patients with bunion deformity. J Foot Ankle Surg. 2007 May-Jun;46(3):149-54.
Coughlin MJ, Jones CP. Hallux valgus: demographics, etiology, and radiographic assessment. Foot Ankle Int. 2007 Jul;28(7):759-77.
Nix S, Smith M, Vicenzino B. Prevalence of hallux valgus in the general population: a systematic review and meta-analysis. J Foot Ankle Res. 2010 Sep 27;3:21.
Glasoe WM, Nuckley DJ, Ludewig PM. Hallux valgus and the first metatarsal arch segment: a theoretical biomechanical perspective. Phys Ther. 2010 Jan;90(1):110-20.
Torkki M, Malmivaara A, Seitsalo S, Hoikka V, Laippala P, Paavolainen P. Surgery vs orthosis vs watchful waiting for hallux valgus: a randomized controlled trial. JAMA. 2001 May 16;285(19):2474-80.
Kaufmann G, Dammerer D, Heyenbrock F, Braito M, Moertlbauer L, Liebensteiner M. Minimally invasive versus open chevron osteotomy for hallux valgus correction: a randomized controlled trial. Int Orthop. 2019 Feb;43(2):343-350.
Donley BG, Vaughn RA, Stephenson KA, Richardson EG. Keller resection arthroplasty for treatment of hallux valgus deformity: increased correction with fibular sesamoidectomy. Foot Ankle Int. 2002 Aug;23(8):699-703.
Giannini S, Faldini C, Nanni M, Di Martino A, Luciani D, Vannini F. A minimally invasive technique for surgical treatment of hallux valgus: simple, effective, rapid, inexpensive (SERI). Int Orthop. 2013 Sep;37(9):1805-13.
Dujela MD, Langan T, Cottom JM, DeCarbo WT, McAlister JE, Hyer CF. Lapidus Arthrodesis. Clin Podiatr Med Surg. 2022 Apr;39(2): 187-206.
Resch S, Stenström A, Reynisson K, Jonsson K. Chevron osteotomy for hallux valgus not improved by additional adductor tenotomy. A prospective, randomized study of 84 patients. Acta Orthop Scand. 1994 Oct;65(5):541-4.
Root M, Orien W, Weed J. Normal and Abnormal Function of the Foot. Vol. 2. Los Angeles: Clinical Biomechanics Corporation; 1977.
Krannitz KW, Fong HW, Fallat LM, Kish J. The effect of cigarette smoking on radiographic bone healing after elective foot surgery. J Foot Ankle Surg. 2009 Sep-Oct;48(5):525-7.
Dux K, Smith N, Rottier FJ. Outcome after metatarsal osteotomy for hallux valgus: a study of postoperative foot function using revised foot function index short form. J Foot Ankle Surg. 2013 Jul-Aug;52(4): 422-5.
Duan X, Kadakia AR. Salvage of recurrence after failed surgical treatment of hallux valgus. Arch Orthop Trauma Surg. 2012 Apr;132(4):477-85.
Aiyer A, Shub J, Shariff R, Ying L, Myerson M. Radiographic Recurrence of Deformity After Hallux Valgus Surgery in Patients With Metatarsus Adductus. Foot Ankle Int. 2016 Feb;37(2):165-71.
No comments:
Post a Comment