Adult Spinal Deformity
Dr. KS Dhillon
Introduction
Adult Spinal Deformity is an idiopathic or degenerative condition of the adult spine. The deformity is in the coronal or sagittal plane. A diagnosis is made with full-length x-rays of the spine. The Initial treatment is usually nonoperative with NSAIDs and physical therapy. Surgical correction of the deformity is indicated for progressive disabling pain that has not responded to nonoperative management, and in patients with progressive neurological deficits.
Epidemiology
Males and females are equally affected and the mean age is 60 years.
Idiopathic scoliosis is more common in the thoracic spine and degenerative scoliosis occurs more commonly in the lumbar spine.
Etiology
There can be a coronal plane imbalance or sagittal plane imbalance. Sagittal plane imbalance is defined as a radiographic sagittal imbalance of more than 5cm. Coronal plane imbalance is defined as lateral deviation of the normal vertical line of the spine of more than 10 degrees.
Degenerative scoliosis results from the asymmetric degeneration of disc space and or the facet joints in the spine. When it occurs in the coronal plane it produces scoliosis and in the sagittal plane, it produces kyphosis or lordosis.
Factors that contribute to loss of sagittal plane balance include, preexisting scoliosis, iatrogenic instability, osteoporosis, and degenerative disc disease.
Classification
There are 2 types of coronal deformity. One is idiopathic (residual) adult scoliosis that results from untreated adolescent idiopathic scoliosis and the other is degenerative (de novo) adult scoliosis. Coronal deformity in the adult can be caused by degenerative changes, can be iatrogenic, or can be caused by paralysis.
In idiopathic (residual) scoliosis the curve follows classic curve patterns. It involves more vertebral segments. The curves are large and it is located in the thoracic spine.
Degenerative (de novo) adult scoliosis lacks classic curve patterns. It involves fewer vertebral segments. The curves are smaller and it involves the lumbar spine.
Presentation
Symptoms
Low back pain is the commonest symptom. It is present in 40% to 90% of the patients. The pain is caused by spondylosis, spine instability or the pain can be from the disc. The pain is more severe and recurrent as compared to the general population.
Spinal stenosis can occur on the concave side of the curve. It can produce neurogenic claudication that would produce pain in the lower extremities and buttocks. Unlike classic claudication, patients with scoliosis and stenosis do not obtain relief of pain with sitting and forward flexion.
Foraminal and lateral recess stenosis is worse in the concavity of the deformity where there is vertebral body rotation and translation. It can produce radicular leg pain and weakness.
Physical examination
Examination will show spinal deformity with thoracic prominence when the patient bends forward. There may be associated muscle weakness.
Imaging
Radiographs
Standing scoliosis x-rays in the coronal and sagittal plane with right and left bending films are taken on a full-length long 36-inch cassette. The bending films help assess curve flexibility and the possibility of surgical correction.
On the AP radiograph, the Cobb angle and coronal balance values are obtained. The coronal balance is calculated using the C7 plumb line (C7PL) and center sacral vertical line (CSVL) (fig 1).
On the lateral radiograph, the sagittal balance is calculated using the C7 plumb line (C7PL). On the lateral radiograph, the pelvic incidence is calculated using sacral slope (SS) and pelvic tilt (PT) values.
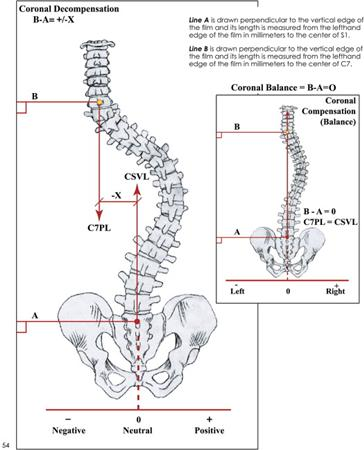
Fig 1
CT scan
A CT scan is useful to identify spinal bony abnormalities. It will also help identify bony deformities such as facet arthrosis.
CT myelogram
A CT myelogram is useful for assessing spinal stenosis, bony anatomy, and rotational deformity.
MRI
In the presence of lower limb pain, an MRI is indicated. It can help identify
central canal stenosis, facet hypertrophy, disc degeneration, pedicular enlargement, and foraminal encroachment.
Treatment
Nonoperative
In patients with coronal curves of less than 30 degrees, the treatment is conservative because such curves rarely progress. The treatment modalities include NSAIDs, tricyclic antidepressants if there is sleep disturbance, physical therapy, corticosteroid injections, and nerve root blocks to treat pain. Bracing can slow progression and reduce discomfort.
Operative
When surgery is necessary, surgical curve correction with instrumented fusion is carried out. It is usually carried out in patients with curves of more than 50 degrees. Surgery is carried out when there is sagittal imbalance, curve progression, intractable back or radicular pain and when there is
cardiopulmonary decline. Thoracic curves of more than 60 degrees affect pulmonary function tests. Thoracic curves of more than 90 degrees can predispose to mortality. Sometimes surgery is carried out for cosmesis.
Posterior only curve correction and instrumented fusion is carried out in patients with thoracic curves of more than 50 degrees and most double structural curves of more than 50 degrees.
A combined anterior and posterior curve correction with instrumented fusion is carried out in patients with isolated thoracolumbar and isolated lumbar curves. Extremely rigid curves will require anterior release.
The aim of surgery is to restore spinal balance, relieve pain and obtain a solid fusion. Worse outcomes is seen in patients with baseline depression and obesity.
The proximal fusion level extends to a neutral and horizontal vertebra above the main curve. The distal fusion extends to L5 if there is no pathology at L5/S1. There is a high failure rate if instrumentation does not extend to the sacrum if there is pathology at L5/S1.
The fusion should be extended to the sacrum when there is pathology at
L5-S1 such as spondylolisthesis, spondylolysis, and facet arthrosis.
A prior laminectomy at L5-S1 would also be an indication for extending the fusion to the sacrum.
A concomitant anterior release and anterior column support through an anterior approach may be needed for better correction of the deformity. The advantage of the long fusion construct is increased stability of the fusion construct and it is less likely to fail.
The disadvantages include an increased risk of pseudoarthrosis, increased surgical time, increased reoperation rate, increased risk of sacral insufficiency fractures, and altered postoperative gait.
The fusion can be extended to the ilium (sacropelvic fusion) if the sacrum is included in fusion involving more than 3 levels.
In osteoporotic patients, cement augmentation can be used. The cement is injected through a fenestrated tap at the end vertebra followed by pedicle screw insertion.
In patients with severe angular deformities, osteotomies are useful to regain sagittal balance. Thirty degrees or more correction can be obtained through Smith-Petersen or pedicle subtraction osteotomies. When osteotomy is carried out intraoperative neuromonitoring is required.
A Smith-Petersen osteotomy (SPO) is carried out for mild to moderate sagittal imbalance that requires correction of up to 10 degrees per level of osteotomy. The prerequisites are that there should be no anterior fusion at the level of osteotomy and there should be adequate disc height and mobility. The correction is at the level of the disc. There is more correction at the lumbar spine due to greater disc height and mobility. The correction is less in the thoracic spine due to lesser disc height and mobility.
In patients with severe sagittal imbalance of more than 12cm requiring correction of 30 degrees to 35 degrees in the lumbar spine, and 25 degrees in the thoracic spine, where anterior fusion is present, pedicle subtraction osteotomy (PSO) is performed. The correction is at the level of the vertebral body and not at the disc.
Vertebral column resection becomes necessary when there is severe sagittal imbalance requiring correction of up to 45 degrees. It is also necessary when there is rigid angular thoracic spine kyphosis, such as that associated with tumors, fractures, or infection. Severe rigid scoliosis and congenital kyphosis would require hemivertebrae resection in the thoracic or lumbar spine.
Anterior procedures are carried out for rigid large curves of more than 70 degrees. Rigid curves are those with no flexibility on side-bending films.
Anterior procedures are also carried out for isolated lumbar or thoracolumbar curves and for anterior interbody fusion at L5/S1 when fusing to the sacrum. Anterior release and fusion are usually combined with posterior instrumentation and fusion.
The disadvantages of anterior procedures are that the surgery is longer if performed on the same day and the complication rates are higher and they are medically more stressful. The advantages are that they increase the stability of L5-S1 long fusion constructs and helps to restore and maintain sagittal and coronal balance.
Surgical Complications
The overall complication rate of adult spinal deformity surgery is about 13.5%. There are 10% major complications that often irreversibly affect the long-term health of the patient. The complication rate is significantly higher when osteotomies, revision procedures, and combined anterior/posterior surgery is performed.
The complications include:
1. Pseudoarthrosis
The incidence of pseudoarthrosis following the surgery is between 5% and 25%. The most common surgical technique associated with pseudoarthrosis is posterior only fusion. The incidence is about 15%. Pseudoarthrosis is most commonly seen at the L5-S1 junction and at the thoracolumbar junction.
The risk factors for pseudoarthrosis include age more than 55 years, hip arthritis, smoking, kyphosis more than 20 degrees, positive sagittal balance of more than 5cm, thoracoabdominal approach, and incomplete lumbopelvic fixation.
2. Dural tear
The incidence of dural tears is about 2.9%.
3. Infection
The incidence of deep wound infection is about 1.5% and superficial wound infection about 0.9%. The risk of infection increases with smoking, diabetes, increasing age, and revision surgery.
4. Implant complication
Implant failure is more likely to occur in bone with lowest ratio of cortical to cancellous bone. Implant failure is the most common cause of reoperation (38.2%) followed by infection (11.8%).
5. Neurologic deficits
Acute neurological deficits can occur in about 1.0% of the patients intraoperatively during deformity correction maneuver. If it is identified on
neurophysiologic monitoring, the instrumentation should be removed, and a wake-up test done. Delayed neurological deficits occurs in about 0.5% of the patients.
Acute neurological deficits can occur due to nerve root injury caused by screw malposition and corrective maneuver.
6. Epidural hematoma
Epidural haematoma occurs in about 0.2% of the patients.
7. Pulmonary embolus
Pulmonary embolism can be seen in about 0.2% of the patients.
8. Deep venous thrombosis
Deep venous thrombosis is seen in about 0.2% of the patients.
9. Deaths
Death as a complication is seen in about 0.3% of the patients.
Prognosis
Worse prognosis is seen in patients in whom the symptoms progress to the side of curve convexity and in patients with sagittal plane imbalance. A sagittal plane balance is the most reliable predictor of clinical symptoms in adult patients with spinal deformity.
Thoracic curves progress more than lumbar curves, lumbar curves more than thoracolumbar curves and thoracolumbar curves more than double major curves. Right thoracic curves progress about 1 degree per year, right lumbar curves about 0.5 degrees per year and thoracolumbar curves about 0.25 degrees per year.
Curves that are less than 30 degrees rarely progress. Curves that are more than 50 deg commonly progress. In patients with preexisting rotational changes progression also occurs.
No comments:
Post a Comment