Flexor Tendon Injuries Of The Hand
Dr. KS Dhillon
Anatomy of Flexor tendons
Muscles
The flexor digitorum profundus arises from the proximal 3/4 of medial and anterior surfaces of the ulna and interosseous membrane. It is inserted at the base of the distal phalanx of the fingers. The medial part (slips to little and ring finger) is innervated by the ulnar nerve (C8, T1) and the lateral part (slips to index and middle finger) is innervated by the anterior interosseous nerve (C8, T1). The ulnar and anterior interosseous arteries provide the blood supply. It functions as a flexor of the distal interphalangeal (DIP) joint and it assists with proximal interphalangeal (PIP) and metacarpophalangeal (MCP) flexion.
Flexor digitorum superficialis (FDS) originates from the medial epicondyle of the humerus, ulnar collateral ligament, coronoid process of the ulna, and superior half of the anterior border of the radius. It is inserted on the bodies of the middle phalanges of fingers. It functions as a flexor of the middle phalanges at the PIP joints of the fingers. It also flexes the proximal phalanges at MCP joint. It is innervated by the median nerve (C7, C8, T1). The arterial supply is provided by the ulnar artery. The FDS to the small finger is absent in 25% of people.
The flexor pollicis longus (FPL) originates from the anterior surface of the radius and adjacent interosseous membrane. It is inserted on the base of the distal phalanx of the thumb. It flexes the phalanges of the thumb. It is located within the carpal tunnel as the most radial structure. It is innervated by the anterior interosseous nerve (C8, T1). The blood supply is provided by the anterior interosseous artery.
The flexor pollicis brevis has 2 heads. The superficial head originates from the flexor retinaculum and tubercles of scaphoid and trapezium. The deep head orginates from the trapezoid and capitate (more medial than superficial head). The flexor pollicis brevis is inserted on the lateral side of base of proximal phalanx of thumb. It functions as a thumb flexor. The superficial head is innervated by the recurrent branch of the median nerve (C8, T1) and deep head is innervated by the deep branch of ulnar nerve.
The arterial supply is from the superficial palmar branch of the radial artery.
The flexor carpi radialis (FCR) originates from the medial epicondyle of the humerus and is inserted on the base of the 2nd metacarpal. It lies close to the median nerve. It flexes and abducts the hand at the wrist. It is innervated by the median nerve (C6, C7). The blood supply is provided by the ulnar artery.
The flexor carpi ulnaris (FCU) originates from the medial epicondyle of the humerus, the olecranon, and the posterior border of the ulna. It is inserted on the pisiform bone, hook of hamate bone, and the 5th metacarpal bone. It flexes and adducts the hand at the wrist. It is innervation by the ulnar nerve (C7, C8). The arterial supply is from the ulnar artery.
Camper chiasm
The tendinous chiasm is situated where tendons of flexor digitorum superficialis and flexor digitorum profundus muscles cross each other.
The FDS tendon enters the A1 pulley and divides into 2 equal halves that rotate laterally and then dorsally. The 2 slips rejoin deep to the FDP tendon over the distal aspect of the proximal phalanx and the palmar plate of the PIP joint at the camper’s chiasm. The 2 slips then insert separately on the volar aspect of the middle phalanx (fig 1).
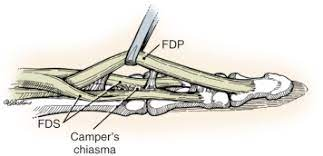
Fig 1.
Pulley system
There are 5 annular pulleys (A1 to A5) in each finger. They are thicker and stiffer than the cruciate pulleys. The A2 and A4 pulleys arise from the periosteum and are important pulleys to prevent flexor tendon bowstringing. The A1, A3, and A5 arise from the volar plate and overlie the MP, PIP, and DIP joints respectively (fig 2). The A1 pulley is most commonly involved in a trigger finger.
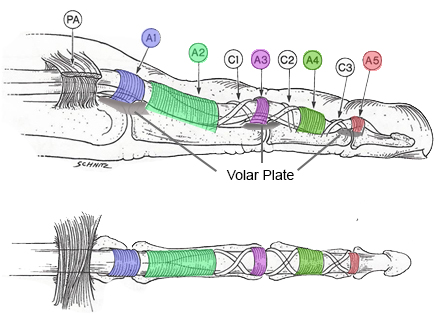
Fig 2.
There are 3 cruciate pulleys (C1 to C3). They are situated at the level of the joints (fig 2). They function to prevent sheath collapse and expansion during digital motion. They facilitate approximation of annular pulleys during flexion.
The thumb contains 3 annular pulleys (A1, Av, A2). The A2 contributes least to the arc of motion of the thumb (fig 3). The Av oblique pulley is the most important pulley to prevent flexor tendon bowstringing (along with the A1 pulley). The oblique pulley (3-5mm) originates at the proximal half of the proximal phalanx. It facilitates full excursion of flexor pollicis longus (FPL) and prevents bowstringing of FPL. Bowstringing will occur if both A1 and oblique pulleys are cut. The blood supply comes from 2 sources. One is by
diffusion through synovial sheaths and direct vascular perfusion outside of synovial sheaths.
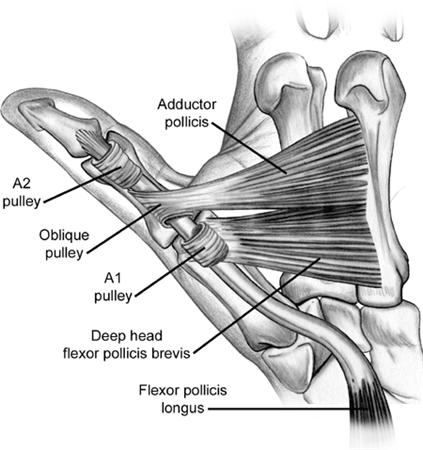
Fig 3
Zones of flexor tendon injuries (fig 4)
Zone 1 is distal to the FDS insertion. Injury to the FDP in this zone produces a Jersey finger. A Jersey finger is a traumatic flexor tendon injury caused by an avulsion injury of the FDP from the insertion at the base of the distal phalanx. On clinical examination, the finger lies in slight extension at the DIP relative to other fingers in the resting position. X-rays may show a bony avulsion if present. Treatment is direct tendon repair or open reduction and internal fixation depending on the presence and size of a bony avulsion.
Zone II extends from the FDS insertion to the distal palmar crease/proximal A1 pulley. In this zone, FDP and FDS are in the same tendon sheath (both can be injured within the flexor retinaculum). The tendons can retract if the vincula are disrupted. The treatment is by direct tendon repair followed by early range of movement exercises (Duran, Kleinert). Passive finger flexion and active extension to an orthosis is carried out. Historically this zone had very poor results but results have improved due to advances in postoperative motion protocols.
Zone III is situated in the palm. It extends from the A1 pulley to the distal aspect of the carpal ligament. Injuries in this zone are often associated with neurovascular injury which carries a worse prognosis. The treatment is by direct tendon repair. Good outcome from direct repair can be expected due to the absence of retinacular structures provided there is no neurovascular injury. An A1 pulley release may be needed to avoid impingement of the repaired tendon on the pulley.
Zone IV is situated in the carpal tunnel. The tendon surgery is often complicated by postoperative adhesions due to close quarters and synovial sheath of the carpal tunnel. The treatment is by direct tendon repair. The
transverse carpal ligament should be repaired in a lengthened fashion if tendon bowstringing is present.
Zone V extends from the carpel tunnel to the forearm. The tendon injury is
often associated with neurovascular injury which carries a worse prognosis.
The treatment is by direct tendon repair.
In the thumb, there are three zones (TI,TII,TIII). The outcome of thumb tendon injuries is different from finger injuries. The early motion protocols do not improve the long-term results. There is a higher re-rupture rate as compared to flexor tendon repair in fingers. The treatment is by direct end-to-end repair of FPL. Zone III should be avoided to prevent injury to the recurrent motor branch of the median nerve.
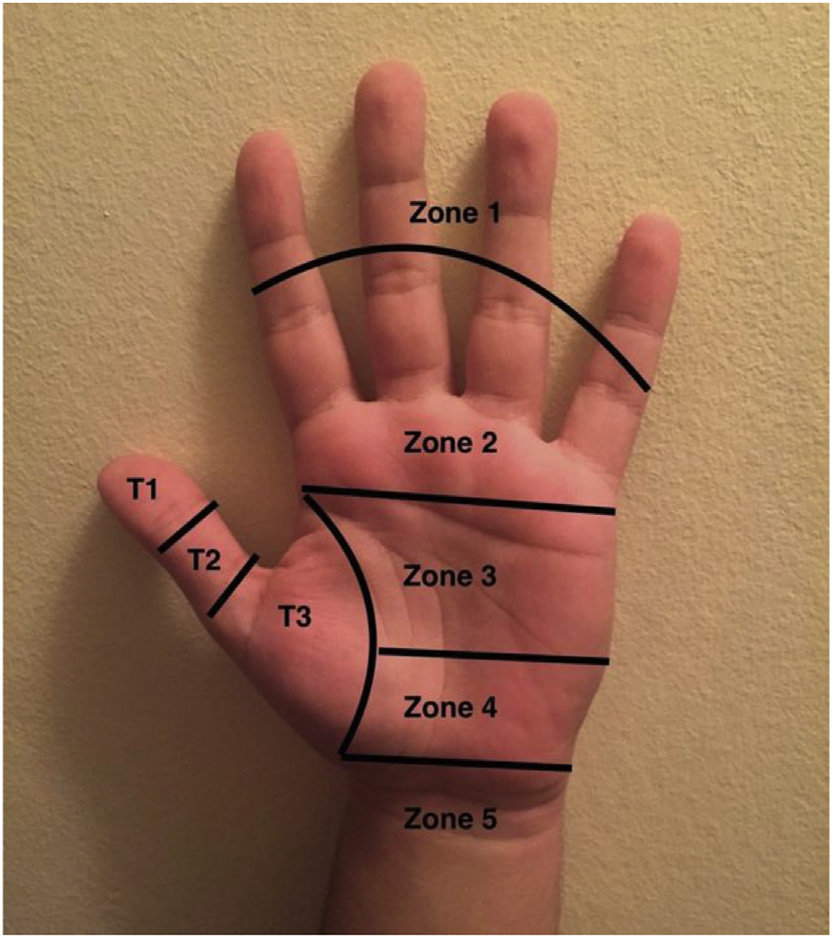
Fig 4
Clinical Presentation
Symptoms of flexor tendon injury include a loss of active flexion strength and motion of the involved digit. Normally passive wrist flexion and extension allows for assessment of the tenodesis effect. Normally wrist extension causes passive flexion of the digits at the MCP, PIP, and DIP joints. Maintenance of extension at the PIP or DIP joints with wrist extension indicates flexor tendon discontinuity. Active PIP and DIP flexion is tested in isolation for each digit.
A neurovascular examination is important given the close proximity of flexor tendons to the digital neurovascular bundles.
X-rays are taken to exclude associated fractures.
Treatment
Nonoperative
Partial lacerations of less than 60% of tendon width can be treated non operatively with wound care and early range of motion exercises.
Operative
Lacerations of more than 60% of tendon width are treated surgically with flexor tendon repair and controlled mobilization.
In patients with failed primary repair and in patients with chronic untreated injuries flexor tendon reconstruction and intensive postoperative rehabilitation are necessary.
In patients with chronic FPL rupture, a FDS of the ringer finger is transferred to the thumb in a single-stage procedure.
Techniques of tendon repair
The indications for flexor tendon repair include a more than 75% laceration of the tendon and equal to or more than 50-60% laceration with triggering. An epitendinous suture at the laceration site is sufficient. There are no
benefits of adding a core suture.
Fundamentals of repair include easy placement of sutures in the tendon,
secure suture knots, smooth juncture of the tendon ends, minimal gapping at the repair site, minimal interference with tendon vascularity, and sufficient strength throughout healing to permit application of early motion stress to the tendon.
The repair should be performed within three weeks of injury, ideally within 2 weeks. Delayed treatment leads to difficulty due to tendon retraction.
Incisions should always cross flexion creases transversely or obliquely to avoid contractures. The tendon handling should be atraumatic to minimize adhesions.
The number of suture strands that cross the repair site is more important than the number of grasping loops. There is a linear relationship between the strength of the repair and the number of sutures crossing the repair. Four to six strands provide adequate strength for early active motion. A high-caliber suture material increases strength and stiffness and decreases gap formation. Locking loops also decrease gap formation. The site of ideal suture placement is 10mm from the cut edge.
Circumferential epitendinous suture improves tendon gliding by reducing the cross-sectional area. It improves the strength of repair by adding 20% to tensile strength. It allows for less gap formation. Simple running suture is recommended.
A repair of the sheath theoretically improves tendon nutrition through the synovial pathway. Clinical studies, however, show no difference with or without sheath repair.
Tendon repairs are weakest between postoperative day 6 and day 12. The
repair usually fails at suture knots. Repair site gaps of more than 3mm are associated with an increased risk of repair failure. Adhesion formation is more common with zone 2 injuries.
Flexor tendon reconstruction
For flexor tendon reconstruction the skin must be supple, sensation intact and there should be adequate vascularity. The passive range of movements of the adjacent joints must be full. The procedure can be a single-stage or two-stage procedure.
A single-stage procedure is only performed if the flexor sheath is pristine and the digit has full ROM.
There are 2 types of two-stage procedures:
1. Hunter-Salisbury
Here in stage I a tendon spacer is placed to create a favorable tendon bed. In stage II, about 3-4 months later, the tendon spacer is retrieved and a tendon graft is placed through the mesothelium-lined pseudosheath.
Proximally pulvertaft weave is done and distally end-to-end tenorrhaphy is carried out. Postoperatively a Kleinert´s splint is applied and after 24 hours finger exercises are started.
2. Paneva-Holevich
In stage I tendon spacer is placed in the flexor sheath, pulleys are reconstructed (as needed), and a loop between the proximal stumps of FDS and FDP is created in the palm.
In stage II the tendon spacer is retrieved, FDS is cut proximally and reflected distally through the pseudosheath and either attached directly to the FDP stump or secured with a button.
The most commonly used tendon for grafting is the palmaris longus. It is however absent in 15% of the population. If a longer graft is necessary the plantaris is used. It is absent in 19% of the population. Other grafts available include extensor digitorum longus to 2nd-4th toes, extensor indicis proprius, flexor digitorum longus to 2nd toe, and FDS.
One pulley should be reconstructed proximal and distal to each joint. Pulley reconstruction should be done first if a tendon graft is being used.
The A2 pulley is important. It is unclear if A4 reconstruction is absolutely necessary. For graft material, the extensor retinaculum synovialized pulley surface provides the least gliding resistance. The palmaris, plantaris, FDS, and flexor tendon allograft can be used as graft material.
First, all scar dorsal to the flexor tendon is excised.
In the encircling technique or around-the-bone technique, a single-loop (Bunnell) or triple loop (Okutsu) technique can be used. The triple loop technique is biomechanically strongest construct.
There are several techniques for the nonencircling reconstruction. These include ever-present-rim (Kleinert), belt-loop (Karev), extensor retinaculum (Lister), and the palmaris longus transplantation through volar plate (Doyle and Blythe) techniques.
Tenolysis
Tenolysis is indicated when there is localized tendon adhesions with minimal to no joint contracture and full passive finger movements. It may also be required if there is a discrepancy between active and passive motion of the fingers after therapy. Tenolysis is carried out after 3 months when the soft tissues have stabilized and there is full passive motion of all joints. While doing tenolysis one has to be careful to preserve A2 and A4 pulleys. Intensive physiotherapy is carried out post-operatively.
Postoperative rehabilitation after tendon repair
Controlled mobilization after the surgery has been the major reason for improved results with tendon repair, especially in zone II. It leads to improved tendon healing biology. It also limits restrictive adhesions and leads to increased tendon excursion.
Immobilization using a splint with wrist and MCP joints in flexion and IP joints in extension is necessary for children and non-compliant patients.
Early passive motion is started using the Duran protocol (active finger extension with patient-assisted passive finger flexion and static splint) or the Kleinert protocol (active finger extension with dynamic splint-assisted passive finger flexion).
Early active motion is also started with moderate force with a dorsal blocking splint limiting wrist extension.
Complications
There are several complications that arise following tendon repairs.
1. Tendon adhesions
Tendon adhesions is the most common complication following flexor tendon repair. The risk is highest with zone 2 injuries. The adhesions are initially treated with physical therapy. If physical therapy does not work tenolysis is performed. Tenolysis is performed 4-6 months after tendon repair if there is a significant loss of excursion.
2. Rerupture
The rerupture rates are between 15-25%. If the scar is less than 1cm, the scar is resected and primary repair is carried out. If the scar is more than
1cm the scar is excised and a tendon graft is performed. If the sheath is collapsed, a Hunter rod is placed, and staged grafting is performed.
3. Joint contracture
A joint contracture is seen in about 17% of the patients. A contracture release has to be carried out sometimes.
4. Swan-neck deformity
Clinical examination reveals resting hyperextension of the PIP joint combined with resting flexion of the DIP joint of the involved digit. It is initially treated with a course of PIP splinting to prevent hyperextension. In progressive cases, volar plate advancement with central slip tenotomy is performed.
5. Trigger finger
Trigger finger is the inhibition of smooth tendon gliding due to mechanical impingement at the level of the A1 pulley. The triggering causes pain, clicking, catching, and locking of the finger. Physical examination shows the presence of active triggering and tenderness at the A1 pulley. Treatment consists of anti-inflammatory medications and steroid injections. In resistant cases surgical release may be necessary.
6. Lumbrical plus finger
Lumbrical plus finger is characterized by extension of the IP joints while attempting to flex the fingers. Clinical examination will show extension of the IP joints of one digit when the fingers are flexed to make a fist. When the symptoms are minimal no treatment is required. When the symptoms affects patients activities surgical treatment is carried out with tenodesis of FDP to terminal tendon or with a lumbrical release.
7. Quadrigia
It is most commonly caused by a functional shortening of the FDP tendon due to over-advancement of the FDP during tendon repair. A more than 1 cm advancement is associated with quadriga. It is characterized by an active flexion lag in fingers adjacent to a digit with a previously repaired FDP tendon. Clinical examination will show the inability to fully flex the fingers of the hand adjacent to the injured finger. If there are minimal symptoms no treatment is reuired. If it affects the patients activities than surgery is carried to release the FDP tendon.
No comments:
Post a Comment