Leg Length Discrepancy
Dr. KS Dhillon
Leg length discrepancy (LLD) is a common condition that may be caused by a congenital defect, disruption of the physis, trauma, or a paralytic disorder. It presents with limb length inequality of varying magnitude.
Diagnosis can be made by clinical measurement with a tape, with block testing, and radiographic scanography. CT scans can be used to calculate LLD in the presence of joint contractures.
Limb length inequality of less than 2 cm at skeletal maturity does not need any treatment. Surgical intervention is indicated for differences of 5 cm or more. Shoe raise is used for inequality of between 2 cm to 5 cm.
Epidemiology
Leg length inequality is common, with 23% of the general population having a discrepancy of 1 cm or more [1]. Ninety percent of normal population has a 5mm LLD. A 2cm LLD occurs in up to 2/3 of the population.
Etiology
The causes of LLD can generally be divided into two broad categories: congenital and acquired. Congenital LLD is due to limb hypoplasia syndromes, the most common of which are the longitudinal deficiency of the fibula; hemihypertrophy syndromes, such as Klippel-Trénaunay-Weber syndrome; or skeletal dysplasias. Acquired causes of LLD include anything that injures or slows the growth of the epiphysis, such as a bony bar due to trauma or infection; shortening, such as that from a fracture with overriding bone fragments; and any systemic condition that results in asymmetric innervation or vascularization.
Classification
LLD can be of two types: Static or progressive. Static is seen in individuals who have a malunion of the femur or tibia. Progressive is seen in individuals who have physeal growth arrest and in individuals with congenital causes of the LLD.
Functional Effects
The functional effects of leg length inequality on gait have been studied. Gait asymmetry requires a leg length inequality of at least 2 cm [2,3]. (3%). Leg length inequalities of 2 cm and less do not seem to alter the kinematics or kinetics of gait [4]. Larger inequalities are associated with greater mechanical work [5], and equalizing limb length improves the symmetry of gait [6].
The effect of gait asymmetry on hip and knee arthrosis, back pain, and scoliosis is not so clear. The association between LLD and back pain has not been established [7-10]. Small leg length inequalities do not appear to increase the incidence of back pain [7,9]. Tjernstrom and Rehnberg [11] reported improvement in back pain in patients who have had lengthening for correction of large (3 to 14 cm) LLD.
There are reports that state that the incidence of scoliosis is higher in patients with leg length inequality [12,13]. If the leg length inequality caused scoliosis, it would be expected that the scoliosis would compensate for the inequality with the convex of the curve toward the short leg, but in one-third of the cases, the opposite is true [14].
The effects of leg length inequality on the lower limbs remains largely speculative. Tjernstrom and Rehnberg[11] reported few lower extremity complaints in patients with LLD. The longer limb will place the hip in 4° to 5° of adduction in an individual with 2 cm leg length inequality, but only with equal weight on each limb and symmetric joint positions. There is no evidence that LLD leads to early hip or knee arthrosis [15].
Clinical assessment
Individuals with LLD are usually asymptomatic. Numerous radiographic and clinical measurements have been used to assess LLD. Clinical assessment includes determination of a level pelvis with the patient standing. Any significant LLD will be obvious, though the location of the inequality may not be apparent. The individual has to stand with both knees and hips extended and in neutral abduction/adduction. A set of blocks of various heights can be placed under the shorter leg till the pelvis is square and the amount of inequality in limb length can be determined. This method is more accurate than measuring the limb length with a tape [16]. A standing anteroposterior (AP) radiograph of the pelvis, with an appropriately sized block under the shorter limb, can confirm the findings.
The Galeazzi test (fig1) can be used to assess significant leg length inequality. The examination is done with the patient supine and the hips and knees flexed. The test is positive if the height of the knees is asymmetrical. It is helpful in determining whether LLD is primarily from the femur or the tibia and in assessing lower limb length in someone who has knee or hip flexion contractures.
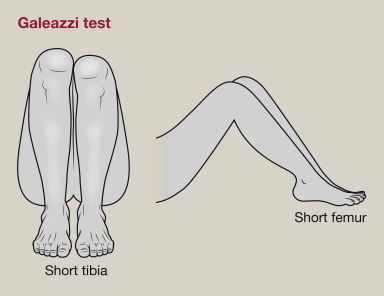
Figure 1. Galeazzi test.
Various radiographic studies have been used to determine LLD. The teleroentgenogram is a single-exposure AP radiograph of the lower limbs with a ruler. It is subject to a magnification error of 5% to 10% at the outer border of the film but it has the advantage of showing coronal (angular) deformities and is not subject to movement errors [15].
Orthoradiography incorporates three separate exposures of the hip, knee, and ankle in an effort to avoid magnification errors. Scanography uses a similar technique, and all three exposures are on one film cassette. Both orthoradiography and scanography are subject to movement errors, and angular deformities cannot be assessed.
All the techniques are inaccurate if the patient has hip or knee flexion contractures, or if the patient flexes the knee or hip asymmetrically at the time of exposure. In patients with hip and knee flexion contractures lateral radiographs, or separate prone radiographs of the femur and tibia with a ruler, can be obtained to assess leg length.
The use of CT scans to assess limb length has now increased. The radiation exposure is less and it is more accurate than conventional radiographic techniques in patients with hip and knee flexion contractures [17]. Ultrasonography is also now used, primarily as a screening tool [18]. Leg-length discrepancy can be reliably determined by ultrasound, although the accuracy is less than that obtained by radiographic methods. Because ultrasound is not limited by radiation hazards, the technique can be used for clinical screening.
A prediction of the ultimate leg length inequality at skeletal maturity will be needed to determine treatment once the current leg length inequality has been measured. The three methods typically used to do this are the growth remaining curve, the arithmetic method, and the Moseley straight-line graph [19]. The multiplier method has also been described recently in which an arithmetic formula is used to determine limb inequality at maturity [20].
The simplest is the arithmetic method [21]. This method assumes that the growth of the distal femur is 1 cm per year, the growth of the proximal tibia is 0.6 cm per year, and skeletal maturity occurs at age 16 for boys and age 14 for girls.
The growth-remaining graphs relate the individuals chronologic age to limb length to determine the growth percentile. With this method, the remaining growth of the tibia or femur can be determined graphically.
Moseley [19] in an effort to combine this information into one graph, incorporated the same data into one straight-line graph. With this technique, several measurements can be plotted on one graph. There is little significant difference between the three techniques [22].
There are several sources of error when leg length inequality at skeletal maturity is determined. An error can occur from radiographic technique, patient position, determination of skeletal maturity, and measurement. Furthermore, growth inhibition may not be constant with age and may worsen or improve with time, leading to underestimation or overestimation of the leg length inequality at maturity [23].
Treatment Methods
Treatment of leg length inequality can be carried out using many different approaches, such as epiphysiodesis, orthotics, lengthening, and shortening. These approaches can be used alone or in combination to achieve equalization of leg lengths.
Leg length inequality of 2 cm or less usually does not produce any functional disability and does not need any treatment. Usually, leg length can be equalized with a shoe lift, and this usually corrects about two-thirds of the leg length inequalities. Up to a 1 cm raise can be inserted in the shoe. For larger leg length inequalities, the shoe has to be built up.
Leg length inequalities of more than 5 cm are difficult to treat with a shoe lift. The shoe looks unsightly, and very often the patient complains of instability with such a large lift. A foot-in-foot prosthesis can be used for larger leg length inequalities. The prosthesis is bulky, and a fixed equinus contracture can develop. Leg lengthening is usually carried out LLD of 5 cm and more.
Epiphysiodesis is a useful procedure that inhibits growth with few complications. The final leg length inequality and the degree of growth inhibition need to be predicted and is subject to errors. The procedure may be unappealing to the patient and family because the procedure effectively shortens the longer leg and is usually done on the uninvolved side.
Epiphysiodesis is very useful in conjunction with limb lengthening for large leg length inequality. By performing an epiphysiodesis, a second or third lengthening can be avoided. For example, if a patient has a 10 cm limb length inequality and has gained 7 cm by lengthening, an appropriately timed epiphysiodesis can result in limb length equality for the final 3 cm discrepancy, without the need for another lengthening.
Phemister [24] described a technique for epiphysiodesis. He removed a section of the epiphysis, then rotated it 90°, and replaced the bone. Currently, the most common technique used for epiphysiodesis is the percutaneous drill epiphysiodesis, done with the aid of an image intensifier. This technique results in physeal closure in 85% to 100% of patients [25-28] with few complications [29]. Scott et al [29] compared the Phemister technique with the percutaneous technique and found the results to be similar. They preferred the percutaneous technique because it is easy to perform and has low morbidity.
Staple epiphysiodesis can also be done, but it is associated with more complications and is a more invasive procedure. The staples are prominent or they tend to back out [30]. Staple epiphysiodesis allows for growth after staple removal.
Percutaneous epiphysiodesis using transphyseal screws have also been used in an effort to provide a reversible method of inhibiting growth with less morbidity.
After skeletal maturity shortening techniques can be used to achieve leg length equality. Shortening can be performed in the proximal femur using a blade plate or hip screw, and in the mid-diaphysis of the femur using a closed intramedullary technique, or in the tibia. Shortening is an accurate technique [31] and involves a much shorter convalescence than the lengthening techniques [31,32]. Quadriceps weakness can occur with femoral shortenings, especially if a mid-diaphyseal shortening of greater than 10% is done [33]. If the femoral shortening is done proximally, no significant weakness would result.
When tibial shortening is done, there may be residual bulkiness of the leg. There are also risks of nonunion and compartment syndrome [34,35]. If tibial shortening is carried out, prophylactic compartment release is recommended. The shortening of the tibia should not exceed 4 to 5 cm in skeletally mature patients.
Bone lengthening is usually done by corticotomy and gradual distraction of the bone fragments. This technique can produce lengthenings of 25% or more. Typically lengthening of 15%, or about 6 cm, is recommended [36]. The extent of lengthening possible depends on patient tolerance, bony consolidation, maintenance of range of motion, and stability of the proximal and distal joints.
There are several fixation devices available for bone lengthening. These include ring fixators with fine wires, monolateral fixators with half pins, and hybrid frames. The monolateral device is easier to apply and is better tolerated by the patient. The disadvantages of monolateral fixation devices include the limitation of the degree of angular correction that can be obtained; the cantilever effect on the pins that may result in angular deformity. This is especially so when lengthening the femur is done in large patients. There is also difficulty in making adjustments without placing new pins. Monolateral fixators appear to have a similar success rate as circular fixators, especially with modest lengthenings of about 20% [37].
For 1 cm of length gain, about 30 days in the fixation device are necessary for both lengthening and consolidation. Generally, femoral lengthenings heal faster than tibial lengthening, as do lengthenings in patients less than 14 years of age. The level of the corticotomy does not seem to have a significant effect in the tibia, and mid-diaphyseal corticotomy appears to be the best in the femur [38].
Other techniques, such as acute lengthening, Wagner technique, and physeal distraction, are used much less commonly to obtain limb length equality. The Wagner technique involves immediate and more rapid lengthening followed by plating and bone grafting. Arron and Eilert [39] and DalMonte and Donzelli [40] found that the Ilizarov technique resulted in fewer complications and does not require an additional procedure for plating and bone grafting. The use of the Ilizarov technique needs fewer procedures but the pain scores are increased and there is a slightly higher complication rate than the Wagner technique.
Acute correction of LLD is difficult to obtain and is limited to about 3 cm. Acute lengthening is done in the mid-diaphysis of the femur or through an innominate osteotomy. The latter is indicated for a patient with primary pelvic asymmetry.
Lengthening can also be done through epiphyseal distraction. This is a less invasive technique and no corticotomy is necessary. However, it can be painful if the physis acutely separates, and it may lead to premature physeal closure and septic arthritis.
Large leg length inequalities can be treated by staged lengthenings or by simultaneous ipsilateral femoral and tibial lengthenings. Additionally, lengthenings can be combined with appropriately timed epiphysiodesis in an effort to produce leg length equality. Staged lengthenings are often used for congenital deficiencies such as fibular hemimelia, in which 15 cm or more may be needed to produce leg length equality. We typically plan for the final lengthening to be completed by age 13 or 14 years and allow at least 3 years between lengthenings.
Lengthening of both the femur and tibia simultaneously can produce soft tissue contractures that require aggressive treatment. Curran et al [41] reported the need for surgical release of soft tissue contractures in 3 of 8 patients they treated with simultaneous ipsilateral tibial and femoral lengthenings.
In an effort to decrease the amount of time, the fixator needs to be worn and to prevent angular malalignment lengthening over an IM nail can be done. The patient has to be skeletally mature. The procedure carries up to 15% risk of osteomyelitis. Furthermore, if premature consolidation occurs, a repeat corticotomy is more difficult [42,43,44].
Complications
Complications of limb lengthenings are common. Complication rates depend on the degree of lengthening, and the surgeon's experience [45]. Complication rates from most series are about one per procedure, and many of these require operative treatment [38,41,46]. Pin site infection is the most common complication. Pin sites are kept clean and dry. If there is excessive discharge, redness, or swelling, antibiotics are used. The presence of periosteal reaction around the pin sites indicates loosening of the pins [47].
In patients with femoral lengthening, the knee range of motion uniformly decreases by an average of 37°. At follow-up, however, the mean loss in the range of motion is usually minimal [48]. Other more serious complications include osteomyelitis, fracture, or joint subluxation. The incidence of these more serious complications is about 25% [45].
Some patients with limb lengthening develop muscle weakness [49,50], pain, and possible physeal inhibition. Physeal inhibition occurs in younger patients with open physis.
Hope et al [51] found little difference in growth velocities before and after bone lengthening. Viehweger et al [52] on the other hand found growth inhibition in the tibia after bone lengthening in children. Unlike pain associated with conventional surgery, pain due to lengthening continues beyond the postoperative period and through the lengthening and consolidation phases,[53] until the fixator is removed.
The use of somatosensory evoked potential monitoring can be useful in preventing neurologic injuries, especially to the peroneal nerve [54]. The use of ultrasound and/or electrical stimulation may decrease the time to consolidation [55].
Reference
Gross RH: Leg length discrepancy: how much is too much? Orthopedics 1:307-310, 1978.
Kaufman KR, Miller LS, Sutherland DH: Gait asymmetry in patients with limb-length inequality. J Pediatr Orthop 16:144-150, 1996.
Liu XC, Fabry G, Molenaers G, et al: Kinematic and kinetic asymmetry in patients with leg-length discrepancy. J Pediatr Orthop 18:187-189, 1998.
Goel A, Loudon J, Nazare A, et al: Joint moments in minor limb length discrepancy: a pilot study. Am J Orthop 26:852-856, 1997.
Song KM, Halliday SE, Little DG: The effect of limb-length discrepancy on gait. J Bone Joint Surg Am 79:1690-1698, 1997.
Bhave A, Paley D, Herzenberg JE: Improvement in gait parameters after lengthening for the treatment of limb-length discrepancy. J Bone Joint Surg Am 81:529-534, 1999.
Grundy PF, Roberts CJ: Does unequal leg length cause back pain? a case-control study. Lancet 2:256-258, 1984.
Gofton JP: Persistent low back pain and leg length disparity. J Rheumatol 12:747-750, 1985.
Soukka A, Alaranta H, Tallroth K, et al: Leg-length inequality in people of working age. the association between mild inequality and low-back pain is questionable. Spine 16:429-431, 1991.
ten Brinke A, van der Aa HE, van der Palen J, et al: Is leg length discrepancy associated with the side of radiating pain in patients with a lumbar herniated disc? Spine 24:684-686, 1999.
Tjernstrom B, Rehnberg L: Back pain and arthralgia before and after lengthening. 75 patients questioned after 6 (1-11) years. Acta Orthop Scand 65:328-332, 1994.
Scheller M: Uber den Einfluss der Beinverkurzung auf die Wirbelsaule. Koln, Inaug Diss, 1964.
Papaioannou T, Stokes I, Kenwright J: Scoliosis associated with limb-length inequality. J Bone Joint Surg Am 64:59-62, 1982.
Moseley CF: Leg length discrepancy. Pediatric Orthopaedics. Lovell WW, Winter RB (eds). Philadelphia, Lippincott Williams & Wilkins, 5th Ed, 2001, chap 28, pp 1107-1108.
Stanitski DF: Limb length inequality: assessment and treatment options. J Am Acad Orthop Surg 7:143-153, 1999.
Lampe HI, Swierstra BA, Diepstraten AF: Measurement of limb length inequality. comparison of clinical methods with orthoradiography in 190 children. Acta Orthop Scand 67:242-244, 1996.
Aaron A, Weinstein D, Thickman D, et al: Comparison of orthoroentgenography and computed tomography in the measurement of limb-length discrepancy. J Bone Joint Surg 74:897-902, 1992.
Terjesen T, Benum P, Rossvoll I, et al: Leg-length discrepancy measured by ultrasonography. Acta Orthop Scand 62:121-124, 1991.
Moseley CF: A straight-line graph for leg-length discrepancies. J Bone Joint Surg Am 59:174-179, 1977.
Paley D, Bhave A, Herzenberg JE, et al: Multiplier method for predicting limb-length discrepancy. J Bone Joint Surg Am 82:1432-1446, 2000.
Westh RN, Menelaus MB: A simple calculation for the timing of epiphyseal arrest: a further report. J Bone Joint Surg Br 63:117-119, 1981.
Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphysiodesis. J Pediatr Orthop 16:173-179, 1996.
Shapiro F: Developmental patterns in lower-extremity length discrepancies. J Bone Joint Surg Am 64:639-651,1982.
Phemister D: Operative arrestment of longitudinal growth in the treatment of deformities. J Bone Joint Surg Am 15:1, 1933.
Gabriel KR, Crawford AH, Roy DR, et al: Percutaneous epiphysiodesis. J Pediatr Orthop 14:358-362, 1994.
Porat S, Peyser A, Robin GC: Equalization of lower limbs by epiphysiodesis: results of treatment. J Pediatr Orthop 11:442-448, 1991.
Timperlake RW, Bowen JR, Guille JT, et al: Prospective evaluation of fifty-three consecutive percutaneous epiphysiodeses of the distal femur and proximal tibia and fibula. J Pediatr Orthop 11:350-357, 1991.
Ogilvie JW, King K: Epiphysiodesis: two-year clinical results using a new technique. J Pediatr Orthop 10:809-811, 1990.
Scott AC, Urquhart BA, Cain TE: Percutaneous vs modified Phemister epiphysiodesis of the lower extremity. Orthopedics 19:857-861, 1996.
May VRJ, Clements EL: Epiphyseal stapling: with special reference to complications. South Med J 58:1203-1207, 1965.
Blair VP III, Schoenecker PL, Sheridan JJ, et al: Closed shortening of the femur. J Bone Joint Surg Am 71:1440-1447, 1989.
Chapman ME, Duwelius PJ, Bray TJ, et al: Closed intramedullary femoral osteotomy. shortening and derotation procedures. Clin Orthop 287:245-251, 1993.
Nordsletten L, Holm I, Steen H, et al: Muscle function after femoral shortening osteotomies at the subtrochanteric and mid-diaphyseal level. a follow-up study. Arch Orthop Trauma Surg 114:37-39, 1994.
Coppola C, Maffulli N: Limb shortening for the management of leg length discrepancy. J R Coll Surg Edinb 44:46-54, 1999.
Kempf I, Grosse A, Abalo C: Locked intramedullary nailing. its applications to femoral and tibial axial, rotational, lengthening, and shortening osteotomies. Clin Orthop 212:165-173, 1986.
Karger C, Guille JT, Bowen JR: Lengthening of congenital lower limb deficiencies. Clin Orthop 291:236-245, 1993.
Maffulli N, Fixsen JA: Distraction osteogenesis in congenital limb length discrepancy: a review. J R Coll Surg Edinb 41:258-264, 1996.
Noonan KJ, Leyes M, Forriol F, et al: Distraction osteogenesis of the lower extremity with use of monolateral external fixation. J Bone Joint Surg Am 80:793-806, 1998.
Aaron AD, Eilert RE: Results of the Wagner and Ilizarov methods of limb-lengthening. J Bone Joint Surg Am 78:20-29, 1996.
DalMonte A, Donzelli O: Comparison of different methods of leg lengthening. J Pediatr Orthop 8:62-64, 1988.
Curran AR, Kuo KN, Lubicky JP: Simultaneous ipsilateral femoral and tibial lengthening with the Ilizarov method. J Pediatr Orthop 19:386-390, 1999.
Simpson AH, Cole AS, Kenwright J: Leg lengthening over an intramedullary nail. J Bone Joint Surg Br 81:1041-1045, 1999.
Paley D, Herzenberg JE, Paremain G, et al: Femoral lengthening over an intramedullary nail. a matched-case comparison with Ilizarov femoral lengthening. J Bone Joint Surg Am 79:1464-1480, 1997.
Gordon JE, Schoenecker PL, Goldfarb CA, et al: Femoral lengthening over a humeral intramedullary nail in preadolescent children. Pediatric Orthopaedic Society of North America, Annual Meeting, Vancouver, BC, May 2000.
Dahl MT, Gulli B, Berg T: Complications of limb lengthening. a learning curve. Clin Orthop 301:10-18, 1994.
Glorion C, Pouliquen JC, Langlais J, et al: Femoral lengthening using the callotasis method: study of the complications in a series of 70 cases in children and adolescents. J Pediatr Orthop 16:161-167, 1996.
Minty I, Maffulli N, Hughes TH, et al: Radiographic features of limb lengthening in children. Acta Radiol 35:555-559, 1994.
Herzenberg JE, Scheufele LL, Paley D, et al: Knee range of motion in isolated femoral lengthening. Clin Orthop 301:49-54, 1994.
Kaljumae U, Martson A, Haviko T, et al: The effect of lengthening of the femur on the extensors of the knee. an electromyographic study. J Bone Joint Surg Am 77:247-250, 1995.
Maffulli N, Fixsen JA: Muscular strength after callotasis limb lengthening. J Pediatr Orthop 15:212-216, 1995.
Hope PG, Crawfurd EJ, Catterall A: Bone growth following lengthening for congenital shortening of the lower limb. J Pediatr Orthop 14:339-342, 1994.
Viehweger E, Pouliquen JC, Kassis B, et al: Bone growth after lengthening of the lower limb in children. J Pediatr Orthop 7:154-157, 1998.
Young N, Bell DF, Anthony A: Pediatric pain patterns during Ilizarov treatment of limb length discrepancy and angular deformity. J Pediatr Orthop 14:352-357, 1994.
Makarov MR, Delgado MR, Birch JG, et al: Intraoperative SSEP monitoring during external fixation procedures in the lower extremities. J Pediatr Orthop 16:155-160, 1996.
Ehrlich MG, Eberson C, Hogan K, et al: The effect of low intensity ultrasound stimulation on consolidation of the regenerate zone in a rat model of distraction osteogenesis. Pediatric Orthopaedic Society, Annual Meeting, Vancouver, BC, May 2000.
No comments:
Post a Comment