Sever Disease
Dr. KS Dhillon
Introduction
Sever disease also known as calcaneal apophysitis is a common cause of heel pain in skeletally immature athletes. It is believed to be due to an overuse injury to the secondary ossification center by a traction apophysitis at the Achilles tendon insertion site on the calcaneus [1]. This condition often coincides with the onset of a pediatric/adolescent patient's rapid growth spurt or due to a sudden increase in sports-related activity, particularly requiring repetitive running and jumping [2].
There is resolution of pain during periods of rest and inactivity. Clinical examination shows tenderness over calcaneal insertion of the Achilles tendon and a positive squeeze test. Diagnosis of Sever disease is clinical and no imaging is required [3]. The course of the disease is self-limiting, and treatment includes activity modification or relative rest. Symptoms can be managed with ice, anti-inflammatory drugs, heel cups or heel lifts, and in severe cases, immobilization [4]. A rehabilitation program focusing on heel cord stretching and strengthening is included in the management plan to both improve symptoms and correct predisposing underlying biomechanical factors.
Etiology
Sever disease is an overuse injury to the calcaneal apophysis due to repetitive strain and microtrauma caused by the force of the strong Achilles tendon. It results in irritation and potential partial avulsion of the relatively soft calcaneal apophysis. The force is increased after increased activity and periods of rapid growth. Occasionally, trauma may lead to a full avulsion fracture. Factors that contribute to the development of Sever disease include increased or excessive sports activity especially sports that require repetitive running and jumping, heel cord tightness, weak ankle dorsiflexion, poorly cushioned or worn-out shoes, and running on hard surfaces. Biomechanical factors that contribute to poor shock absorption such as forefoot varus, genu varum, pes cavus, or pes planus can also predispose an individual to this condition [5].
Epidemiology
Sever disease usually occurs during the period of rapid growth in active adolescent patients between 9 and 12 years of age. It is the most common cause of heel pain in this age group. Symptoms can be unilateral or bilateral. Upto 60% of cases present with bilateral pain. Sever disease is more common in males, presenting most frequently at a median age of 12 years for males and 11 years for females. It is usually seen in individuals who are involved in sports that require repetitive running and jumping such as basketball, soccer, track, cross-country, and gymnastics. Risk factors for the disease include general risk factors for overuse injury such as long or year-round activities, poorly fitting or worn-out footwear, and poor training mechanics. Biomechanical factors such as poor heel cord flexibility, pes cavus, pes planus, genu varum, or forefoot varus can predispose the patients to develop this disease [1,6].
Pathophysiology
The posterior part of the calcaneus develops as a secondary ossification center that provides attachment for the Achilles tendon (fig 1). During the early adolescent growth spurt, bone growth exceeds the ability of the muscle-tendon unit to stretch sufficiently to maintain previous flexibility. This in turn leads to increased tension across the unossified or incompletely ossified apophysis. The apophysis is the weakest point in the muscle-tendon-bone-attachment and therefore it is at risk for overuse injury from repetitive stress. Excessive and repetitive traction from the Achilles tendon results in microtrauma and chronic irritation causing thickening and pain at the apophysis [6].
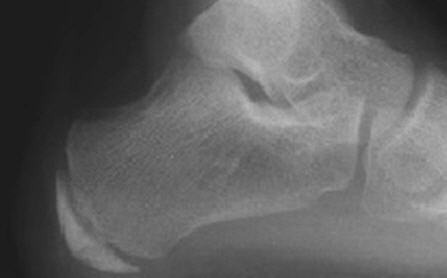
Fig 1.
History and Physical Examination
An active adolescent presents with unilateral or bilateral heel pain that is worse during and after activity, especially running and jumping. It is seen often in the setting of a recent growth spurt or starting a new sport/training. There is usually no history of preceding trauma. The pain improves with rest and typically is absent in the morning. The pain can progress in severity and limit activity. Physical examination will show tenderness and mild swelling at the tendoachilles insertion on the heel. Passive ankle dorsiflexion can produce pain. Pain is reproduced with compression of the posterior calcaneus and aggravated by standing on tiptoes (Sever sign) [3,[7].
Evaluation
Sever disease is a clinical diagnosis. Radiographs are usually not needed. In patients with atypical presentation where the pain is very severe or persistent, radiographs are needed to rule out infection, neoplasm, or an occult fracture.
In patients with Sever disease, plain radiographs may show fragmentation, sclerosis, or increased density of the calcaneal apophysis. These changes, however, can also be seen in normal variants. Bilateral imaging is necessary to delineate osseous abnormality versus normal variants in the individual patient [3,7].
Differential Diagnosis
The differential diagnosis includes:
Achilles Tendon Injuries
Calcaneus Fractures
Osteomyelitis
Tarsal Condition
Treatment
Sever disease is a self-limiting condition that resolves with maturation and closure of the apophysis. The treatment is conservative. There is no role of surgery in the treatment of Sever disease.
The following non-operative options are available for treatment:
Rest/periods of inactivity (guided by pain)-- This may also include staying away from sports until symptoms subside.
Orthotic use/casting-- Immobilization including periods of casting or use of a CAM boot may be necessary depending on the severity of the symptoms.
Heel cups or heel pads
Achilles tendon stretching
Ice application-- Before and after sporting activity
NSAIDs
Footwear should be well-maintained and up-to-date. A rehabilitation program is essential and it should include heel cord stretching in addition to dorsiflexor strengthening exercises. If the pain does not respond to conservative measures, a walking boot or short-leg cast may be used for a short period. Symptoms usually disappear within 6 to 12 months and a complete resolution occurs with apophyseal closure. There are no long-term complications, and the prognosis is usually excellent [4,8].
Prognosis
Recurrence of pain is relatively common but symptoms can be expected to resolve after the closure of the calcaneal apophysis. Symptoms do not persist after the patient reaches skeletal maturity.
References
James AM, Williams CM, Haines TP. Health related quality of life of children with calcaneal apophysitis: child & parent perceptions. Health Qual Life Outcomes. 2016 Jun 24;14:95.
Hart E, Meehan WP, Bae DS, d'Hemecourt P, Stracciolini A. The Young Injured Gymnast: A Literature Review and Discussion. Curr Sports Med Rep. 2018 Nov;17(11):366-375.
Davison MJ, David-West SK, Duncan R. Careful assessment the key to diagnosing adolescent heel pain. Practitioner. 2016 May;260(1793):30-2, 3.
Howard R. Diagnosing and treating Sever's disease in children. Emerg Nurse. 2014 Sep;22(5):28-30.
McSweeney SC, Reed L, Wearing S. Foot Mobility Magnitude and Stiffness in Children With and Without Calcaneal Apophysitis. Foot Ankle Int. 2018 May;39(5):585-590.
Launay F. Sports-related overuse injuries in children. Orthop Traumatol Surg Res. 2015 Feb;101(1 Suppl): S139-47.
Manusov EG, Lillegard WA, Raspa RF, Epperly TD. Evaluation of pediatric foot problems: Part II. The hindfoot and the ankle. Am Fam Physician. 1996 Sep 01;54(3):1012-26, 1031.
James AM, Williams CM, Haines TP. Heel raises versus prefabricated orthoses in the treatment of posterior heel pain associated with calcaneal apophysitis (Sever's Disease): a randomised control trial. J Foot Ankle Res. 2010 Mar 02;3:3.
No comments:
Post a Comment