Clay-shoveler’s fracture
Dr. KS Dhillon
Introduction
The clay shoveler’s fracture was first described by Reginald Dalton McKellar HallClay [1]. Shoveler's fracture is a relatively rare spinous process avulsion fracture that is seen in patients with neck trauma [2-4]. Treatment is usually conservative [3]. In patients where neck pain persists, surgical excision can be considered. Most often, the spinous processes of the C7 and T1 vertebrae are affected. The mechanism of trauma is repetitive, forceful shear pull of the upper back muscles on the relatively long and slender spinous processes, ultimately leading to fatigue fractures. In the past, this condition was an occupational injury mainly seen in laborers shoveling heavy loads. Now it is mostly seen in athletes or seen as recreational injuries and also from trauma following motor vehicle accidents.
Mechanism of Injury
Any violent type of hyper-flexion of the neck in which the inter-spinous ligament remains intact may result in a clay shoveler’s fracture [5]. Nowadays, the injury is most commonly seen following a road traffic accident as the neck muscles suddenly go into spasm during deceleration [6]. More obscure mechanisms have been described in the literature. These include a clay shoveler’s fracture secondary to rock climbing [7], golfing [8], and even during a Wii game [9].
Epidemiology
This condition is rare. It occurs due to direct trauma to the posterior spinous process or indirect trauma caused by sudden muscular/ligamentous pull in flexion or extension of the neck.
It is most commonly seen at C7 but can affect C6 to T3. It usually occurs midway between the spinous tip and lamina. The risk factors include labourers, racket or contact sports, and motor vehicle accidents.
Etiology
The fracture usually occurs in isolation following the trauma. Other orthopaedic injuries to consider are lamina fractures and facet dislocations.
Presentation
There is a sudden onset of pain between the shoulder blades or the base of the neck following the trauma. The neck movements are reduced.
Physical examination will show localized swelling and tenderness over the fracture site. Flexion and extension of the cervical spine is reduced. A neurovascular examination has to be carried out to exclude neurovascular injury.
Imaging
Cervicothoracic x-rays are taken. Both the AP and lateral views are obtained. Lateral views (fig 1) are taken in both flexion and extension. In the lateral view, the fracture line is usually obliquely oriented with the fragment displaced posteroinferior. In the AP view a double spinous process shadow is suggestive of a displaced fracture.
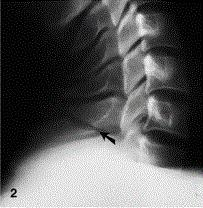
Fig 1.
A CT scan is a method of choice for the diagnosis of this fracture. Routine
CT imaging is carried out in high-energy trauma patients. The clinical criteria for CT imaging are:
altered consciousness
midline spinal pain or tenderness
impaired cervical spine motion
lower cranial nerve paresis
motor paresis
The fracture is best seen on the lateral view.
An MRI is usually not required in isolation. It would be required if there is neurological deficit.
Treatment
The treatment for clay shoveler’s fracture is conservative with NSAIDs, rest, and immobilization in hard collar for comfort. The outcome of conservative treatment is excellent with high union rates.
Surgery will be indicated in patients where conservative treatment has failed and there is persistent pain with nonunion.
Complications
Complications that can occur include chronic pain and neck stiffness
Prognosis
The prognosis is generally good in patients with stable injury in isolation.
It is very rarely associated with neurological injury and the union rates are high.
Conclusion
The patient demographic, mechanism of injury, and diagnostic investigations have changed since the clay shoveler’s fracture was first described by McKellar Hall. The management, however, remains the same. Originally it occurred following low-energy injury in the undernourished. The modern-day clay shoveler’s fracture is most commonly caused by high-energy deceleration trauma due to motor vehicle accidents or sports injuries. The modality of radiographic diagnosis has also changed with the increasing use of CT scans. In addition, the use of MRI to demonstrate bony injury is becoming more commonplace in children and adolescents. The management plan advised in the 1930s remains the same i.e pain relief and rest from aggravating physical activity.
References
Toman E, Beaven A, Harland S, Porter K. Clay-shoveler’s fracture: A snapshot. Trauma. 2016;18(3):186-189. doi:10.1177/1460408616640998
Posthuma de Boer J, van Wulfften Palthe AF, Stadhouder A, Bloemers FW (2016) The Clay Shoveler's Fracture: A Case Report and Review of the J Emerg Med 51: 292-297.
Kang DH, Lee SH (2009) Multiple spinous process fractures of the thoracic vertebrae (Clay-Shoveler's Fracture) in a beginning Golfer: a case report. Spine 34: 534-537.
Yamaguchi KT Jr, Myung KS, Alonso MA, Skaggs DL (2012) Clay-shoveler's fracture equivalent in Spine 37: 1672-1675.
Thomas LPJr., John HHJr. Harris & Harris' radiology of emergency medicine, Philadelphia, PA: Lippincott Williams & Wilkins, 2013.
Lee P, Hunter TB, Taljanovic M. Musculoskeletal colloquialisms: how did we come up with these names? Radiographics 2004; 24: 1009–1027.
Kaloostian PE, Kim JE, Calabresi PA, et al. Clay-shoveler's fracture during indoor rock climbing. Orthopedics 2013; 36: e381–e383.
Kim SY, Chung SK, Kim DY. Multiple cervical spinous process fractures in a novice golf player. J Korean Neurosurg Soc 2012; 52: 570–573.
Brown CN, McKenna P. A Wii-related clay-shoveler's fracture. Sci World J 2009; 9: 1190–1191.
No comments:
Post a Comment