Occipitocervical Instability
Dr. KS Dhillon
Introduction
The occipitocervical junction is a unique, complex, biomechanical interface between the cranium and the upper cervical spine [1]. Craniocervical instability can be congenital or due to trauma, infections, tumors, and inflammatory conditions [2-5].
Occipitocervical instability can present with disabling pain, cranial nerve palsy, paralysis, or even sudden death. Stabilization with fusion is needed to prevent these complications. Occipitocervical fusion can be a technically challenging procedure. Occipitocervical fixation is carried out to avoid injuring the nerve root, the spinal cord, and the vertebral artery and to obtain rigid fusion [6]. Hypoplasia or absence of the occipital bone and co-morbidities that would prevent the operative procedure or the prone positioning are contraindications for occipitocervical fusion [7].
There have been advances in operative techniques and instrumentation techniques for occipitocervical fusion. The procedure has evolved from simple autograft on lay fusion techniques to sublaminar wiring techniques and, recently to rigid occipital plating with bicortical screws [8-15].
Anatomy and biomechanics
There are 2 separate groups of ligaments that play a vital role in maintaining the stability of the occipitocervical junction. The first group consists of the anterior and posterior atlanto-occipital ligaments, the articular capsule ligaments, and two lateral atlanto-occipital ligaments that attach the cranium to the atlas (Fig. 1) [16,17].
The anterior atlanto-occipital ligament is a continuation of the anterior longitudinal ligament. The posterior atlanto-occipital ligament extends from the posterior border of the foramen magnum to the posterior atlantal arch. The cruciate ligament also contributes to the stability of this joint.
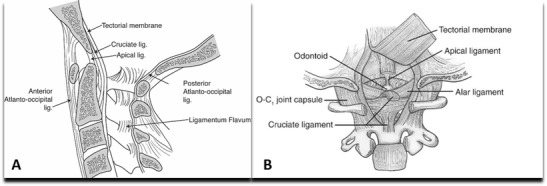
Fig 1.
The second groups of ligaments include the apical ligament, the alar ligaments, the tectorial membrane, and the ligamentum nuchae (Fig. 1) [16-18]. They also provide craniocervical stability. The alar ligaments are paired structures. They consist of two components: the atlanto alar and the occipital alar. They connect the tip of the odontoid to the occipital condyles and the lateral masses of the atlas. They are the main restraints for axial rotation. The tectorial membrane is a continuation of the posterior longitudinal ligament. It runs from the dorsal surface of the odontoid to the ventral surface of the foramen magnum and resists hyperextension [16-18].
Occipitocervical dissociation (OCD) occurs following complete or near complete disruption of the ligamentous structures between the occiput and the upper cervical spine. Extreme forces in hyperflexion, hyperextension, and lateral flexion alone or in combination can result in this injury. The prominent force responsible for producing OCD is usually hyperextension which results in the rupture of the tectorial membrane. Incompetence of the alar ligaments and tectorial membrane allows anterior dislocation of the cranium on the upper cervical spine.
Epidemiology
About 15-30% of cervical spine injuries occur at the occipitocervical junction. Traumatic occipitocervical instability has been identified in 19% of fatal cervical injuries.
Acquired occipitocervical instability is seen most frequently in patients with Down syndrome. It is usually asymptomatic and identified while screening for surgery or screening for special olympic participation.
Etiology
Occipitocervical instability is also known as atlanto-occipital dissociation (AOD) and occipitocervical dislocation. There are 2 types of occipitocervical instability i.e traumatic and acquired.
The traumatic type results from high-energy trauma leading to translation or distraction injuries that destabilize the occipitocervical junction. The head most often displaces anteriorly.
The acquired type is due to bony dysplasia or ligament and soft-tissue laxity. There can be associated atlantoaxial instability as seen in Down syndrome patients. There can be associated neurologic deficit and vertebral or carotid artery injuries.
Classification
There are 2 types of classification for occipitocervical instability namely the Traynelis classification and the Harbourview classification. The Traynelis classification is based on the direction of displacement and the Harbourview classification is based on the degree of instability.
Traynelis Classification
Type 1- Anterior occiput dislocation
Type II- Longitudinal dislocation
Type III- Posterior occiput dislocation
Harbourview Classification System
Stage I- Minimal or non-displaced, unilateral injury to craniocervical ligaments- stable.
Stage II- Minimally displaced, but MRI demonstrates significant soft-tissue injuries. Stability may be based on traction test- Stable or Unstable
Stage III- Gross craniocervical misalignment- Harris lines >2 mm beyond acceptable limits- Unstable
Clinical presentation
The most common cause of OCD is high-speed motor vehicle accidents and striking of pedestrians by motor vehicles [19,20]. OCD is more common among children. The injury is three times more common in children than in adults [21]. A horizontal articular surface and laxity of the ligamentous structures, combined with the presence of a relatively large head and a higher effective fulcrum in the pediatric cervical spine may account for these differences. There is often concurrent head, spinal cord, or multisystem traumatic injuries in patients with OCD because of the severe force involved in producing the injury. Neurological injury from AOD can often lead to sudden death secondary to brainstem injury [22]. Neural injury may be direct due to traction or compression, or indirect, secondary to cerebrovascular injury leading to ischemia [23-26].
Patients who have vertebral artery insufficiency at this level may exhibit Wallenberg syndrome which consists of ipsilateral defects of cranial nerves V, IX, X, and XI; ipsilateral Horner syndrome; dysphagia; and cerebellar dysfunction [23-26]. Respiratory compromise resulting from brainstem compression often makes mechanical ventilation necessary and this can make definitive neurologic assessment difficult.
Survivors of OCD often have neurological impairment including lower cranial nerve deficits, and unilateral or bilateral sensory and motor deficits, cruciate paralysis, or even quadriplegia [23-26]. Neurogenic shock may also be present. It should be appropriately recognized and managed to ensure hemodynamic stability.
Up to 20 % of patients with AOD may have a normal neurological examination at presentation with severe neck pain as the only symptom [23-26]. Any patient involved in high-energy trauma should be suspected of having OCD, irrespective of clinical findings. Appropriate precautionary measures should be taken until the diagnosis is ruled out.
Diagnosis
Plain films of the cervical spine are the first imaging ordered in patients with cervical trauma. The recommended views include AP, lateral, and odontoid views. Injuries to the upper cervical spine are difficult to detect with plain radiographs for several reasons. These include the parallax effect at the occipitocervical junction and obscuration due to mastoid air cells [27].
Lateral cervical X-rays when performed should be evaluated to determine instability such as Powers’ ratio, X-line method, condylar gap method, basion-dens interval (BDI), and basion-axial interval (BAI) [28,29].
The Powers ratio (fig 1) is equal to A-B/CD where A-B is the distance from the basion to the posterior arch and C-D is the distance from the anterior arch to the opisthion (median point on the posterior margin of the foramen magnum). A ratio of 1 is normal. If it is more than 1.0 there is anterior dislocation. If the ratio is less than 1.0 there is posterior atlanto-occipital dislocation, odontoid fracture, or a ring of atlas fracture.

Fig 1.
In Harris's rule of 12 the basion-dens interval and basion-posterior axial interval are measured. A distance of more than 12 mm suggests occipitocervical dissociation (fig 2).
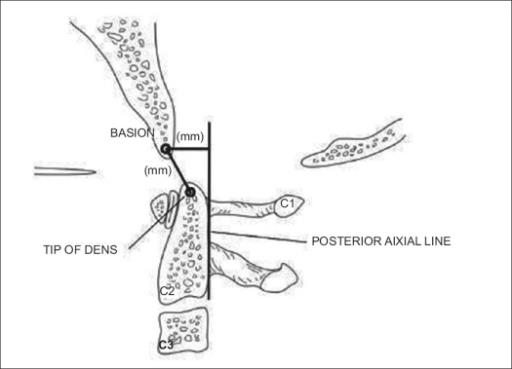
Fig 2.
The radiographic findings in patients with OCD may be subtle or even absent on initial films [30-33]. The use of Harris lines on plain X-rays is often recommended for the diagnosis of OCD. The presence of MRI findings such as signal abnormalities affecting the tectorial membrane, alar and transverse ligaments, or occipitoatlantal joint capsule may also indicate the presence of OCD. Further evaluation with a CT scan can be carried out [23,24,34,35].
Multidetector computed tomography (MDCT) is the imaging modality of choice in an awake symptomatic patient. It is proven to be more sensitive and specific than cervical spine radiographs in detecting spinal cord injury [36]. MDCT of the spine is commonly used as a routine screening test for cervical spine injury and allows for more accurate Harris line measurements. The relevant anatomy is visualized 99.75 % of the time with CT as compared to 39 to 84 % of the time with plain films [27]. It also enables the examiner to visualize the occipitocervical and atlantoaxial joints directly to assess for subluxation.
Direct assessment of condyle to C1 interval (CCI) on a sagittal and coronal CT scan may be more reliable than other radiological measurements to diagnose OCD [27,35,37,38]. Earlier studies suggested a cutoff of ≥2 mm [27] and 2.5 mm [38] as abnormal in adults. Martinez-del-Campo et al [37] proposed a cutoff for the CCI of 1.5 mm and the condylar sum of 3.0 mm as more accurate with 100 % sensitivity and specificity and no false negatives. The study also showed that the cutoff of 2.0 and 2.5 mm had higher false-negative rates of 13.6 and 22.7 %, respectively.
A study by Pang et al [35] found that the normal CCI was 1.28 ± 0.26 mm and they proposed a CCI ≥4 mm as diagnostic for AOD with a sensitivity and specificity of 100 % compared with other standard diagnostic tests.
In children CCI determined on CT has the highest diagnostic specificity and sensitivity for AOD and should be considered the investigation of choice for diagnosing OCD [35].
An MRI will show increased T2-weighted signal intensity within the occiput-C1 and C1-C2 articulations [23,24,35]. Definitive evidence of disruption of the alar and tectorial ligaments can sometimes be seen on the MRI. Evaluation of the spinal cord and brainstem parenchyma can reveal injuries ranging from mild edema to the presence of intraspinal hematoma or even transection. Epidural fluid collections are commonly seen, as is the presence of subdural hematoma.
Treatment and outcomes
Improvement in the maintenance of hemodynamic and respiratory stability at the scene of injury and stabilization of the neck with the proper application of a rigid cervical collar at the scene of injury and during transfer to the hospital had led to an increasing number of these patients surviving this injury that was once considered fatal [21,23,24,37]. More recent series have reported mortality rates as low as 0% in patients who were diagnosed and appropriately treated [25]. If the diagnosis of OCD is delayed by a mean of 2 days (range 1–15 days), almost 40 % of the patients suffer from profound neurological deterioration [24].
Once the diagnosis has been confirmed, neck immobilization with a rigid collar should be maintained until definitive surgical intervention can be performed. The use of cervical traction in the treatment of patients with OCD is controversial with contradictory opinions in various studies. There is a 10% risk of neurological deterioration in patients on cervical traction [32,39-42]. The most appropriate form of provisional stabilization is also controversial and it depends on several factors such as the timing of surgery, the degree of initial displacement, and the patient’s neurologic status, body habitus, and associated injuries. The possible options include rigid cervical collar immobilization, use of halo immobilization, and taping of the head to sandbags [39]. With nonoperative treatment, neurological worsening can occur in upto 50 % of the patients [39].
Cranio-cervical fixation is the treatment of choice in most cases of traumatic OCD [39]. Posterior occipitocervical fusion is the procedure of choice. This can be achieved by using a variety of techniques such as posterior wiring and structural grafting, Ransford loop fixation with wiring or plate/rod, and screw fixation with structural grafting [43,44]. Electrodiagnostic monitoring and continued provisional stabilization are necessary for turning patients with this highly unstable injury into a prone position. The development of rigid fixation has led to increasingly successful outcomes [43-45]. Wire or cable fixed rods or loops only provided semi-rigid fixation. With modern segmental screw-based constructs successful fusion can be obtained in over 90 % of patients [43,45].
Occipitocervical fusion is carried out through a posterior midline incision with the patient in a prone position. Mayfield retractor is used to obtain proper craniocervical alignment. Preoperative O-C2 angle is established with lateral fluoroscopy prior to draping. Deep dissection is then carried out.
If performing C1 lateral mass screw fixation it is proper to work within the safe zone and not to dissect above the posterior arch of C1 more than 1 cm lateral to the midline to avoid injury to the vertebral artery. The posterior instrumented fusion is usually performed from the occiput to C3. The occipital plates usually allow for 3 or 4 total screws with adjustable rod holders. The occipital screws are unicortical to avoid injury to the venous sinus. Major dural venous sinuses are located just below the external occipital protuberance. The safe zone for occipital screws is located within an area measuring 2 cm lateral and 1 cm inferior to the external occipital protuberance along the superior nuchal line. C1 lateral mass screws often skipped due to angle at the base of the skull which makes it more difficult to place a rod. A unilateral screw may be inserted to provide some rotational stability to the C1 ring. C2 fixation can be carried out with a screw in the pars, pedicle, or lamina. For C3 fixation standard lateral mass screws are aimed cephalad and lateral to avoid the vertebral artery. Bone grafting and removal of boney fragments compressing neurovascular structures will be required. Complications include nonunion and bleeding from the internal carotid artery or vertebral artery injury.
Treatment outcomes in survivors of occipitocervical dissociation depend on the following [23,24,25,27]:
Type and severity of associated injuries especially intracranial injuries and cerebrovascular injury.
The severity of neurologic deficit.
The timeline with which the diagnosis of craniocervical dissociation is recognized.
Missed diagnosis of OCD is the most important factor associated with poor outcomes in patients sustaining this injury and is higher in patients with other associated significant injuries and reliance on X-rays alone for initial diagnosis of OCD [24,25,27,46].
Conclusion
OCD is a devastating injury. It is more prevalent than was originally thought. It produces significant morbidity and mortality if left unrecognized. The availability of high-resolution CT has facilitated the diagnosis due to better visualization of the craniocervical junction. Recognition of newer diagnostic criteria for OCD, especially abnormal condylar separation on a high-resolution MDCT, has made it easier to recognize and reduce the incidence of missed diagnosis and its untoward sequel. A high index of suspicion following high-impact trauma with early recognition and prompt surgical intervention can lead to good clinical outcomes. Posterior occipitocervical fusion and instrumentation remains the treatment of choice.
References
J.R. Vender, P.J. Houle, S. Harrison, et al. Occipital-cervical fusion using the Locksley intersegmental tie bar technique: long-term experience with 19 patients Spine J, 2 (2002), pp. 134-141.
C.A. Dickman, S.M. Papadopoulos, V.K.H. Sonntag, et al. Traumatic occipitoatlantal dislocations J Spinal Disor, 6 (1993), pp. 300-313.
F.H. Shen, D. Samartzis, L.G. Jenis, et al. Rheumatoid arthritis: evaluation, surgical management of the cervical spine Spine J, 689 (2004), p. 700.
L. Labler, K. Eid, A. Platz, et al. Atlanto-occipital dislocation: four case reports of survival in adults and review of the literature Eur Spine J, 13 (2) (2004), pp. 172-180.
H. Koller, U. Holz, A. Assuncao, et al. Traumatic Atlantooccipital Dislocation Critical Review: Diagnosis, Classification and Treatment, and Explanative Case Report. European J of Trauma 2006; 32: 271–9. 3- Abumi K, Avadhani A, Manu A, et al. Occipitocervical fusion Eur Spine J, 19 (2010), pp. 355-356.
A. Vaccaro, M. Lim, J. Lee Indications for surgery and stabilization techniques of the occipito-cervical junction Injury Int J Care Injured, 36 (2005), pp. SB44-SB53.
C.G. Randazzo, B. LeBude, J. Ratliff, et al. Occiput–Cervical Fixation Spine Trauma, Part 1, 119 (2010), p. 127.
K. Abumi, A. Avadhani, A. Manu, et al. Occipitocervical fusion Eur Spine J, 19 (2010), pp. 355-356.
J.J. Baskin, C.A. Dickman, V.K.H. Sonntag. Occipitocervical fusion H.R. Winn, R.G. Dacey (Eds.), Youmans Neurological Surgery, Saunders, Philadelphia (2004), pp. 4655-4670.
N.A. Ebraheim, H. Elgafy, R. Xu. Bone graft harvesting from iliac and fibular donor sites: techniques and complications J Am Acad Orthop Surg, 9 (2001), pp. 210-218.
K. Abumi, T. Takada, Y. Shono, et al. Posterior occipitocervical reconstruction using cervical pedicle screws and plate-rod systems Spine, 24 (1999), pp. 1425-1434.
A. Faure, E. Bord, R. Monteiro da Silva, et al. Occipitocervical fixation with a single occipital clamp using inverted hooks Eur Spine J, 7 (1998), pp. 80-83.
V. Heidecke, N.G. Rainov, W. Burkert Occipito-cervical fusion with the cervical Cotrel-Dubousset rod system Acta Neurochir, 140 (1998), pp. 969-976.
P. Korovessis, P. Katonis, A. Aligizakis, et al. Posterior compact Cotrel-Dubousset instrumentation for occipitocervical, cervical and cervicothoracic fusion Eur Spine J, 10 (1998), pp. 385-394.
P. Paquis, V. Breuil, M. Lonjon, et al. Occipitocervical fixation using hooks and screws for upper cervical instability Neurosurgery, 44 (1999), pp. 324-331.
Martin MD, Bruner HJ, Maiman DJ. Anatomic and biomechanical considerations of the craniovertebral junction. Neurosurgery. 2010;66:2–6. doi: 10.1227/01.NEU.0000365830.10052.87.
Tubbs RS, Hallock JD, Radcliff V, et al. Ligaments of the craniocervical junction. J Neurosurg Spine. 2011;14:697–709. doi: 10.3171/2011.1.SPINE10612.
Yuksel M, Heiserman JE, Sonntag VK. Magnetic resonance imaging of the craniocervical junction at 3-T: observation of the accessory atlantoaxial ligaments. Neurosurgery. 2006;59:888–92.
Traynelis VC, Marano GD, Dunker RO, Kaufman HH. Traumatic atlanto-occipital dislocation. Case report. J Neurosurg. 1986;65:863–70. doi: 10.3171/jns.1986.65.6.0863.
Werne S. Studies in spontaneous atlas dislocation. Acta Orthop Scand Suppl. 1957;23:1–150.
Bucholz RW, Burkhead WZ. The pathological anatomy of fatal atlanto-occipital dislocations. J Bone Joint Surg Am. 1979;61:248–50.
Fisher CG, Sun JC, Dvorak M. Recognition and management of atlanto-occipital dislocation: improving survival from an often fatal condition. Can J Surg J Can de Chir. 2001;44:412–20.
Horn EM, Feiz-Erfan I, Lekovic GP, Dickman CA, Sonntag VK, Theodore N. Survivors of occipitoatlantal dislocation injuries: imaging and clinical correlates. J Neurosurg Spine. 2007;6:113–20. doi: 10.3171/spi.2007.6.2.113.
Bellabarba C, Mirza SK, West GA, et al. Diagnosis and treatment of craniocervical dislocation in a series of 17 consecutive survivors during an 8-year period. J Neurosurg Spine. 2006;4:429–40. doi: 10.3171/spi.2006.4.6.429.
Mendenhall SK, Sivaganesan A, Mistry A, Sivasubramaniam P, McGirt MJ, Devin CJ. Traumatic atlantooccipital dislocation: comprehensive assessment of mortality, neurologic improvement, and patient-reported outcomes at a Level 1 trauma center over 15 years. Spine J : Off J N Am Spine Soc. 2015;15:2385–95.
Sweet J, Ammerman J, Deshmukh V, White J. Cruciate paralysis secondary to traumatic atlantooccipital dislocation. J Neurosurg Spine. 2010;12:19–21. doi: 10.3171/2009.8.SPINE08496.
Dziurzynski K, Anderson PA, Bean DB, et al. A blinded assessment of radiographic criteria for atlanto-occipital dislocation. Spine. 2005;30:1427–32. doi: 10.1097/01.brs.0000166524.88394.b3.
Lee C, Woodring JH, Goldstein SJ, Daniel TL, Young AB, Tibbs PA. Evaluation of traumatic atlantooccipital dislocations. AJNR Am J Neuroradiol. 1987;8:19–26.
Rojas CA, Bertozzi JC, Martinez CR, Whitlow J. Reassessment of the craniocervical junction: normal values on CT. AJNR Am J Neuroradiol. 2007;28:1819–23. doi: 10.3174/ajnr.A0660.
Eismont FJ, Bohlman HH. Posterior atlanto-occipital dislocation with fractures of the atlas and odontoid process. J Bone Joint Surg Am. 1978;60:397–9.
Gabrielsen TO, Maxwell JA. Traumatic atlanto-occipital dislocation; with case report of a patient who survived. Am J Roentgenol Radium Therapy, Nucl Med. 1966;97:624–9. doi: 10.2214/ajr.97.3.624.
Pang D, Wilberger JE., Jr Traumatic atlanto-occipital dislocation with survival: case report and review. Neurosurgery. 1980;7:503–8. doi: 10.1227/00006123-198011000-00017.
Woodring JH, Selke AC, Jr, Duff DE. Traumatic atlantooccipital dislocation with survival. AJR Am J Roentgenol. 1981;137:21–4. doi: 10.2214/ajr.137.1.21.
Garrett M, Consiglieri G, Kakarla UK, Chang SW, Dickman CA. Occipitoatlantal dislocation. Neurosurgery. 2010;66:48–55. doi: 10.1227/01.NEU.0000365802.02410.C5.
Pang D, Nemzek WR, Zovickian J. Atlanto-occipital dislocation—part 2: the clinical use of (occipital) condyle-C1 interval, comparison with other diagnostic methods, and the manifestation, management, and outcome of atlanto-occipital dislocation in children. Neurosurgery. 2007;61:995–1015.
Ryken TC, Hadley MN, Walters BC, et al. Radiographic assessment. Neurosurgery. 2013;72(Suppl 2):54–72. doi: 10.1227/NEU.0b013e318276edee.
Martinez-Del-Campo E, Kalb S, Soriano-Baron H, et al. Computed tomography parameters for atlantooccipital dislocation in adult patients: the occipital condyle-C1 interval. J Neurosurg Spine. 2016;24(4):535–45.
Gire JD, Roberto RF, Bobinski M, Klineberg EO, Durbin-Johnson B. The utility and accuracy of computed tomography in the diagnosis of occipitocervical dissociation. Spine J : Off J N Am Spine Soc. 2013;13:510–9. doi: 10.1016/j.spinee.2013.01.023.
Theodore N, Aarabi B, Dhall SS, et al. The diagnosis and management of traumatic atlanto-occipital dislocation injuries. Neurosurgery. 2013;72 Suppl 2:114–26.
Evarts CM. Traumatic occipito-atlantal dislocation. J Bone Joint Surg Am. 1970;52:1653–60.
Levine AM, Edwards CC. Traumatic lesions of the occipitoatthop Relat Res. 1989;(239):53–68.
Watridge CB, Orrison WW, Arnold H, Woods GA. Lateral atlantooccipital dislocation: case report. Neurosurgery. 1985; 17:345–7. doi: 10.1227/00006123-198508000-00021.
Garrido BJ, Puschak TJ, Anderson PA, Sasso RC. Occipitocervical fusion using contoured rods and medial offset connectors: description of a new technique. Orthopedics. 2009;32. doi:10.3928/01477447-20090818-11.
Lu DC, Roeser AC, Mummaneni VP, Mummaneni PV. Nuances of occipitocervical fixation. Neurosurgery. 2010;66:141–6. doi: 10. 1227/01.NEU.0000365744.54102.B9.
Abumi K, Takada T, Shono Y, Kaneda K, Fujiya M. Posterior occipitocervical reconstruction using cervical pedicle screws and plate-rod systems. Spine. 1999;24:1425–34. doi: 10. 1097/00007632-199907150-00007.
Blackwood NJ., III Atlo-occipital dislocation: a case of fracture of the atlas and axis, and forward dislocation of the occiput on the spinal column, life being maintained for thirty-four hours and forty minutes by artificial respiration, during which a laminectomy was performed upon the third cervical vertebra. Ann Surg. 1908;47:654–8. doi: 10.1097/00000658-190805000-00003.
No comments:
Post a Comment