Piriformis Syndrome
Dr. KS Dhillon
Introduction
Yeoman first described piriformis syndrome in 1928 as periarthritis of the anterior sacroiliac joint. Piriformis syndrome is a condition that is characterized by sciatic symptoms (leg pain) due to extrapelvic sciatic nerve compression at the hip. The sciatic nerve entrapment occurs at the level of the ischial tuberosity. There are multiple factors potentially contributing to piriformis syndrome. The clinical presentation is fairly consistent. The patients usually report pain in the gluteal/buttock region that can shoot, burn or ache down the back of the lower limb. Additionally, there can be numbness in the buttocks and tingling sensations along the distribution of the sciatic nerve.
The sciatic nerve runs just adjacent to the piriformis muscle. The piriformis functions as an external rotator of the hip. Whenever the piriformis muscle is inflamed or irritated it can affect the sciatic nerve, leading to sciatica-like pain. The diagnosis of piriformis syndrome is difficult. It is based on good clinical history and examination. Other conditions that can produce symptoms similar to piriformis syndrome include lumbar canal stenosis, disc prolapse, discitis, or pelvic pathology [1,2].
Anatomy
Piriformis is a muscle of the gluteal region that lies deep to the gluteus maximus. It belongs to a group of six short external rotators of the hip, i.e. gemellus superior, obturator internus, gemellus inferior, quadratus femoris, and obturator externus. It arises from the anterior aspect of the sacrum at the level of about S2 through S4, sacrotuberous ligament, and periphery of the greater sciatic notch. It inserts onto the apex of the greater trochanter, posterosuperior to the insertion site of the conjoined tendon of gemellus superior, obturator internus, and gemellus inferior (fig1).
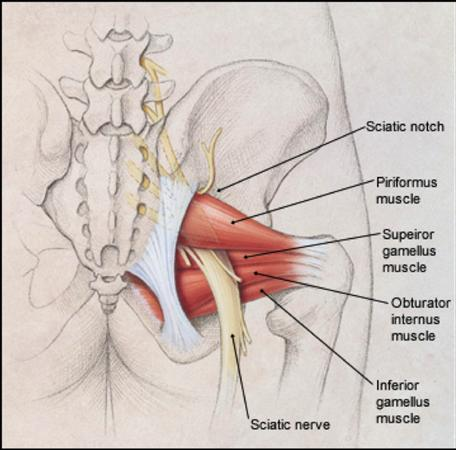
Fig 1.
The muscle divides the greater sciatic foramen into two foramina (suprapiriform and infrapiriform). The superior gluteal artery and nerve leave the pelvis through the suprapiriform foramen. The sciatic nerve, inferior gluteal nerve and artery, posterior femoral cutaneous nerve, and the nerve to quadratus femoris (L4-S1) leave the pelvis through the infrapiriform foramen.
It produces lateral rotation of the hip when the hip is extended (that is when standing), abduction of the hip when it is flexed, and aids slightly in tilting the pelvis laterally. Also aids in tilting the pelvis posteriorly by pulling the sacrum down towards the thigh [3].
Etiology
The sciatic nerve gets entrapped anterior to the piriformis muscle or posterior to the gemelli-obturator internus complex at the level of the ischial tuberosity. The piriformis muscle can be stressed due to poor body mechanics over a period of time or an acute injury with the forceful internal rotation of the hip. There are anatomic anomalies that may contribute to compression of the nerve, including a bipartite piriformis, direct invasion by a tumor, anatomical variations of the course of the sciatic nerve, or an inferior gluteal artery aneurysm.
There are several causes of piriformis syndrome including the following [2]:
Trauma to the buttock or hip area.
Piriformis muscle hypertrophy which is often seen in athletes during periods of increased weightlifting.
Sitting for prolonged periods that is often seen in taxi drivers, office workers, and bicycle riders.
Anatomic anomalies: Bipartite piriformis muscle, sciatic nerve course, and branching variations with respect to the piriformis muscle. In more than 80% of the population, the sciatic nerve courses deep to and exits inferiorly to the piriformis muscle [4]. Early division of the sciatic nerve into its tibial and common peroneal components can predispose patients to piriformis syndrome, with the branches passing through and below the piriformis muscle or above and below the muscle [5].
Epidemiology
Piriformis syndrome is known to be responsible for 0.3% to 6% of all cases of low back pain and/or sciatica. There are about 40 million new cases of low back pain and sciatica annually. With this, the incidence of piriformis syndrome would be about 2.4 million per year. The majority of cases occur in middle-aged patients. The ratio of male to female patients being affected is about 1:6 [2].
Pathophysiology
The piriformis muscle is innervated by nerve branches coming off L5, S1, and S2. When the piriformis muscle is inflamed, overused, or irritated, it leads to irritation of the adjacent sciatic nerve, which runs very close to the center of the muscle.
Sciatic nerve entrapment occurs anterior to the piriformis muscle or posterior to the gemelli-obturator internus complex. The piriformis can be stressed due to poor body posture over a period of time or some acute injury that results in a sudden and strong internal rotation of the hip [6].
History and Physical examination
Patients with piriformis syndrome often present with the following symptoms:
Pain in the buttocks that is worsened by hip movements
Chronic pain in the buttock and hip area
Pain when getting out of bed
Inability to sit for a prolonged time
They often present with symptoms of sciatica. It can be difficult to differentiate the origin of the radicular pain secondary to spinal pathology from that of piriformis syndrome. The pain can radiate into the back of the thigh and the leg at the L5 or S1 dermatomes [7].
There can be mild to moderate tenderness around the sciatic notch. The patient's symptoms can be reproduced by performing flexion, adduction, and internal rotation of the hip (FAIR test).
The FAIR test is done with the patient in the supine position. Then the patient is asked to flex the hip and move it along the midline. At the same time, the examiner rotates the lower leg. This maneuver will apply tension to the piriformis muscle leading to pain
Evaluation
The diagnosis of piriformis syndrome is primarily clinical and is one of exclusion. Physical examination involves attempts to perform stretching maneuvers to stress the piriformis muscle. Manual pressure around the sciatic nerve can help to reproduce the symptoms.
Some of these stretching maneuvers include:
FAIR maneuver - flexion, adduction, internal rotation of the hip.
Freiberg maneuver- forceful internal rotation of the extended thigh.
Pace maneuver- resisted abduction and external rotation of the thigh.
Beatty maneuver- deep buttock pain produced by the side-lying patient holding a flexed knee several inches off the table.
Facet arthropathy, herniated disc, lumbar muscle strain, and spinal stenosis have to be excluded. Ultrasound, MRI, CT, and EMG are useful for the exclusion of these conditions. Electrophysiology will show the presence of H waves. Magnetic resonance neurography may show the presence of irritation of the sciatic nerve just adjacent to the sciatic notch.
Treatment
Treatment includes the use of muscle relaxants, NSAIDs, and physical therapy which entails stretching the piriformis muscle, and range of motion exercises. Steroid Injections around the piriformis muscle can help reduce pain and inflammation. Botulinum toxin has been used to help relieve symptoms. The duration of pain relief is however short-lived, and repeat injections are required [8].
When conservative treatment fails then surgery is necessary. Release of the piriformis tendon and sciatic neurolysis is carried out during surgery. Benson and Schutzer performed such a procedure in 14 patients with an average symptom duration of 38 months. All their patients had piriformis syndrome secondary to trauma. They reported that 11 patients had excellent outcomes, and 4 had good results [9].
Differential Diagnosis
The differential diagnosis of piriformis syndrome includes [10]:
Lumbosacral radiculopathy
Lumbosacral spine sprain
Lumbosacral spondylolisthesis
Lumbosacral spondylolysis
Hamstring injury
Lumbosacral disc injuries
Lumbosacral discogenic pain syndrome
Lumbosacral facet syndrome
Sacroiliac joint injury/dysfunction
Inferior gluteal artery aneurysm or pseudoaneurysm
Malignancy/tumors
Arteriovenous malformations
Prognosis
Many patients with piriformis syndrome will show symptomatic improvement after trigger-point injections. When the injections are combined with rehabilitation exercises, then recurrences are rare.
Patients who undergo surgery may take a few months to return to full activity.
Complications
When surgery is carried out the following complications can occur:
Infection
Bleeding
Sciatic nerve injury
Conclusion
Piriformis syndrome is a painful and debilitating condition that may arise due to anatomic variations. Diagnosis is usually difficult due to limited objective clinical findings and research. However, once the diagnosis is made, prompt management is critical for the patient's quality of life. Currently, the literature favors surgical resection over injections for refractory pain. Correct and early diagnosis is critical in determining best management practices.
References
Siddiq MAB. Piriformis Syndrome and Wallet Neuritis: Are They the Same? Cureus. 2018 May 10;10(5):e2606.
Chang A, Ly N, Varacallo M. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Sep 4, 2022. Piriformis Injection.
Kendal, McCreary, Provance; Muscle Testing and Function with Posture and Pain;4th Edition; Piriformis muscle and its relationship to Sciatic Pain; Page No 365.
Cassidy L, Walters A, Bubb K, Shoja MM, Tubbs RS, Loukas M. Piriformis syndrome: implications of anatomical variations, diagnostic techniques, and treatment options. Surg Radiol Anat. 2012 Aug;34(6):479-86.
Smoll NR. Variations of the piriformis and sciatic nerve with clinical consequence: a review. Clin Anat. 2010 Jan;23(1):8-17.
Huang ZF, Yang DS, Shi ZJ, Xiao J. [Pathogenesis of piriformis syndrome: a magnetic resonance imaging-based comparison study]. Zhonghua Yi Xue Za Zhi. 2018 Jan 02;98(1):42-45.
Hopayian K, Danielyan A. Four symptoms define the piriformis syndrome: an updated systematic review of its clinical features. Eur J Orthop Surg Traumatol. 2018 Feb;28(2):155-164.
Safarpour Y, Jabbari B. Botulinum toxin treatment of pain syndromes- an evidence based review. Toxicon. 2018 Jun 01;147:120-128.
Benson ER, Schutzer SF. Posttraumatic piriformis syndrome: diagnosis and results of operative treatment. J Bone Joint Surg Am. 1999 Jul. 81(7):941-9.
Cass SP. Piriformis syndrome: a cause of nondiscogenic sciatica. Curr Sports Med Rep. 2015 Jan;14(1):41-4.
No comments:
Post a Comment